
Remember me



The incidence and prevalence of end-stage renal disease (ESRD) in Taiwan are among the highest in the world (United States Renal Data System, 2022). The main reasons for the high prevalence of ESRD in Taiwan include societal aging, the growth in the number of patients with chronic diseases such as diabetes and hypertension (Wang et al., 2021), the use of inappropriate kidney-related medications (Rasool et al., 2020), and the low rate of kidney transplantation (KT; Tsai et al., 2022). ESRD impacts negatively on patients, their families, and society and consumes significant medical resources (Hashmi et al., 2023). Alongside improving patient quality of life, KT is considered the optimal treatment for ESRD and is cost-effective in comparison to other related treatments (Abramyan & Hanlon, 2023).
KT involves the transplantation of a healthy kidney from a donor to a recipient. Depending on the source of the kidney, KTs are classified as either living-donor KTs or deceased-donor KTs (Mayo Clinic, 2023). KTs can improve the survival rate of patients with ESRD, and patients receiving a KT often experience fewer symptoms of kidney disease (Dembowska et al., 2022). The 5-year patient survival rates for living-donor and deceased-donor KTs have been reported as 97.6% and 95.7%, respectively, for recipients aged 18–34 years, and 84.4% and 72.5%, respectively, for recipients aged ≥ 65 years (Lentine et al., 2023). Between 2000 and 2009, 81.3% of patients in Taiwan who survived KT did not return for long-term dialysis within 5 years of their KT surgery (National Health Research Institutes & Taiwan Society of Nephrology, 2022). However, the 5-year survival rate of patients receiving dialysis alone has been reported to be 44% (United States Renal Data System, 2022). Thus, KT is the preferred and gold-standard treatment modality for ESRD (Lang et al., 2022).
KT willingness refers to the willingness and behavioral intention of patients with ESRD to undergo a KT. The willingness of patients to undergo a KT is fundamental to KT referral and treatment processes. Willingness is the quality or state of being prepared to do something, and positive willingness is a good predictor of behavior actualization. Strong willingness becomes more stable over time and makes an individual less susceptible to external efforts to change related behaviors (Conner & Norman, 2022).
Rates of chronic kidney disease, hemodialysis, and willingness to undergo a KT among patients with ESRD vary significantly by country. For patients with chronic kidney disease, rates of KT willingness were found to be 54% in the United States (Ilori et al., 2015), 69% in India (Kaur et al., 2019), and 67% in Ghana (Boima et al., 2021). For hemodialysis patients, rates of KT willingness were found to be 69% in Saudi Arabia (Alansari et al., 2017), 63% in Turkey (Kalender et al., 2015), 63% in Tanzania (Mzee et al., 2020), 60% in Pakistan (Ali et al., 2023), 73.3% in Morocco (Kabbali et al., 2014), and 35%–46% in China (Qiao et al., 2016; Tan et al., 2017). For patients with ESRD, rates of KT willingness were found to be 66.7% in Nigeria (Takure et al., 2016) and 16% in Taiwan (Chang, 2013). The willingness of patients in countries in East Asia to undergo a KT is relatively low compared to other regions and countries. Although Taiwan is home to numerous patients with ESRD, the proportion of those willing to undergo a KT is low. Moreover, although Taiwanese dependent on dialysis in 2019 numbered 86,840, only 9.0% were registered on a KT wait list (National Health Research Institutes & Taiwan Society of Nephrology, 2022). Therefore, factors affecting patients' KT willingness merit further investigation.
Researchers have explored relationships between sociodemographics and willingness to undergo a KT. Previous studies have revealed that patients who are male (Calvo-Calvo et al., 2018; Kim et al., 2023), younger (Alansari et al., 2017; Tan et al., 2017), more highly educated (Alansari et al., 2017; Hamilton et al., 2017), single (Alansari et al., 2017; Hamilton et al., 2017), employed (Tan et al., 2017), and financially well-off (Ilori et al., 2015; Qiao et al., 2016) as well as those who have been on dialysis for shorter periods (Alansari et al., 2017; Qiao et al., 2016) tend to be more willing to undergo a KT. However, some studies have reported unemployed people as being more likely to receive a KT (Calvo-Calvo et al., 2018; Hamilton et al., 2017). However, other potential factors of influence on KT willingness such as patient sources of information on KT (Ilori et al., 2015) and KT-related religious beliefs (Doerry et al., 2022; UT Southwestern Medical Center, 2022) have yet to be clarified. Therefore, the relationship between sociodemographics and KT willingness requires further exploration to help healthcare professionals provide services that are person centered and culturally appropriate.
Although several studies have explored knowledge of and attitudes toward KT among patients with kidney disease, the relationships among knowledge, attitudes, and willingness have not been examined. In Ilori et al. (2015), the vast majority (79.8%) of the patients with kidney disease self-reported their knowledge of KT as “below” average. Also, Alansari et al. (2017) found 61% of the hemodialysis patient participants had “poor” or “very poor” knowledge of KT. Similarly, Boima et al. (2021) reported that approximately 90% of participants rated their knowledge of KT as “below average” or “average,” and Mzee et al. (2020) found only 62.8% of participants had any awareness of KT. The above studies demonstrate a general lack of knowledge regarding KT among patients receiving dialysis. Conversely, one study found 77% of patients had knowledge of KT (Kalender et al., 2015), whereas other studies have revealed positive attitudes toward KT among a majority of participants (Boima et al., 2021; Mzee et al., 2020). However, a systematic literature review by Navaneethan and Singh (2006) identified generally negative attitudes toward KT among African American patients. Another study pointed out that attitudes were more negative and KT willingness was lower among patients aged ≥ 60 years (Alansari et al., 2017). These conflicting findings highlight the need for further investigation of the KT knowledge and attitudes of patients with ESRD and of the influence of these two factors on KT willingness.
Uncertainty persists regarding the significant factors associated with KT willingness, and studies on KT willingness and associated factors among Taiwanese patients with ESRD are scarce. Therefore, this study was designed to examine the KT willingness of patients receiving dialysis and associated influencing factors.
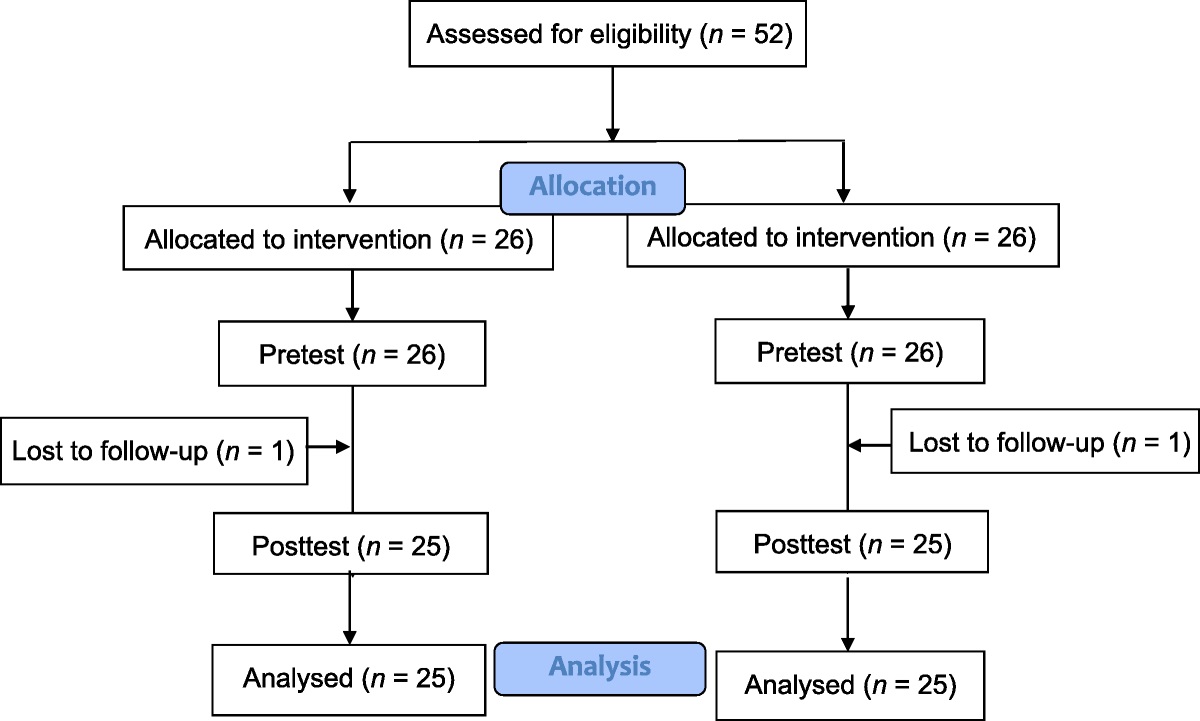
Methods Study Design and ParticipantsIn this cross-sectional study, patients from the dialysis department of one medical center in Taiwan were recruited as participants. An estimated minimum sample size of 157 was calculated using G*Power Version 3.1.9.2 with the following conditions: effect size f2 (medium) of 0.15, alpha level of .05, power of .9, and 12 predictors (Cohen, 2013). All of the participants were recruited in the Department of Nephrology and Dialysis at the study hospital using convenience sampling. Two hundred fourteen questionnaires were distributed, and 209 valid questionnaires were collected (valid response: 97.7%).
The inclusion criteria were as follows: (a) diagnosed with ESRD by a physician and having received hemodialysis on a regular basis for more than 3 months, (b) aged 20–65 years (Taiwan law stipulates kidney recipients must be younger than 66 years; Jih Sun Health Foundation, ROC, 2022), and (c) clear cognition and the ability to communicate in written or spoken Mandarin or Taiwanese. The exclusion criteria were as follows: (a) patients diagnosed with contraindications to KT (e.g., malignancy, severe cardiovascular disease, coagulation disorders, chronic respiratory failure, heart failure, psychiatric disease, severe congenital malformations of the urinary tract, AIDS) and (b) the presence of a speech impairment or refusal to complete the questionnaire.
InstrumentsThe questionnaire, including three scales (as described below), sociodemographics, and disease history, was developed based on related studies (Alansari et al., 2017; Ilori et al., 2015; Qiao et al., 2016). Five clinical experts and academics specializing in kidney disease were invited to review the content validity of the questionnaire items using a 4-point scale (1 = inappropriate to 4 = very appropriate; Gray & Grove, 2020). The content validity index values of the KT knowledge scale, KT attitude scale, and KT willingness scale were .89, .90, and 1.0, respectively. Next, a pilot test of the questionnaire was administered to 15 patients.
Kidney transplantation knowledge scaleThe KT knowledge scale consists of 12 true/false items in the domains of KT evaluation (five items), registration criteria (one item), surgical procedures and sequelae (four items), and regulations (two items: “After receiving KT, a patient may still encounter problems such as infections, rejection, and malignant tumors” and “Renal transplant registries should be performed in multiple hospitals to ensure that registry data are valid”). Correct and incorrect answers are respectively scored 1 and 0, with the total possible score ranging from 0 to 12 and higher scores indicating better KT knowledge. Difficulty levels for the items were .13–.87, and the item discrimination indices were .31–.92 (all > .3), indicating satisfactory discrimination power for the scale (Kumar et al., 2021). The Kuder–Richardson Formula 20 reliability coefficient of the scale was .87.
Kidney transplantation attitude scaleThe KT attitude scale consists of 11 items. A principal component analysis was used to conduct an exploratory factor analysis of construct validity. Two major constructs were identified: attitudes toward transplant surgery (six items; e.g., adequate knowledge of KT, ability to discuss with family members, family support, attending surgical education courses) and attitudes toward negative transplant effects (five items; e.g., concerns about being too old, the cost, unsuccessful surgery, rejection). The total variance was 54.74%, and the Kaiser–Meyer–Olkin value was .802. Each item was rated on a bipolar 5-point Likert scale (−2 = strongly disagree to 2 = strongly agree), with the total possible score ranging from −22 to 22 and higher scores indicating more-positive attitudes toward KT. The Cronbach's α coefficient of the scale in this study was .80.
Kidney transplantation willingness scaleThe KT willingness scale consists of four items related, respectively, to KT registration, deceased-donor KT, live-donor KT, and KT. Responses to each item range from strongly disagree (1) to strongly agree (5), with the total possible score for the scale ranging from 4 to 20 and higher scores indicating greater KT willingness. The Cronbach's α coefficient of the scale in this study was .95.
Sociodemographics and Disease HistoryThe sociodemographic variables considered in this study included gender, age, educational level, marital status, employment status, financial status, religious beliefs, and sources of KT information. Disease history information included the type and duration of dialysis.
Data CollectionThe study period ran from November 25, 2019, to January 31, 2020. The researchers obtained consent to conduct this study from the Director of the Department of Nephrology and Dialysis at the study hospital. Eligible participants were screened for inclusion and invited to participate by one researcher on the study team. After obtaining participants' verbal consent, the purpose of the study, data collection methods, anonymity, and participant rights were explained. The participants were asked to complete the questionnaire at home and return it to the dialysis center nurse at their next visit.
Ethical ConsiderationsThis study was approved by the ethics review committee of Far Eastern Memorial Hospital (No. 108146-E). Participation was voluntary, and the participants had the right to interrupt, stop, or withdraw from the study without affecting their quality of care. Data were kept strictly confidential and were used for this study only.
Data AnalysisData were analyzed using IBM SPSS Statistics 25.0 (IBM Inc., Armonk, NY, USA). The descriptive statistics in this study are presented in terms of counts, percentages, means, and SDs. Pearson's product–moment correlation, independent-samples t test, and one-way analysis of variance were used to examine the relationships between independent variables and dependent variables of interest. In addition, a multiple regression analysis with the enter method was used to examine the predictive power on KT willingness of sociodemographics, disease history, knowledge, and attitudes. In the regression analysis, assumptions of normality, linearity, independence of residuals, and multicollinearity were all met. For all of the analyses, the significance criterion was set to p < .05.
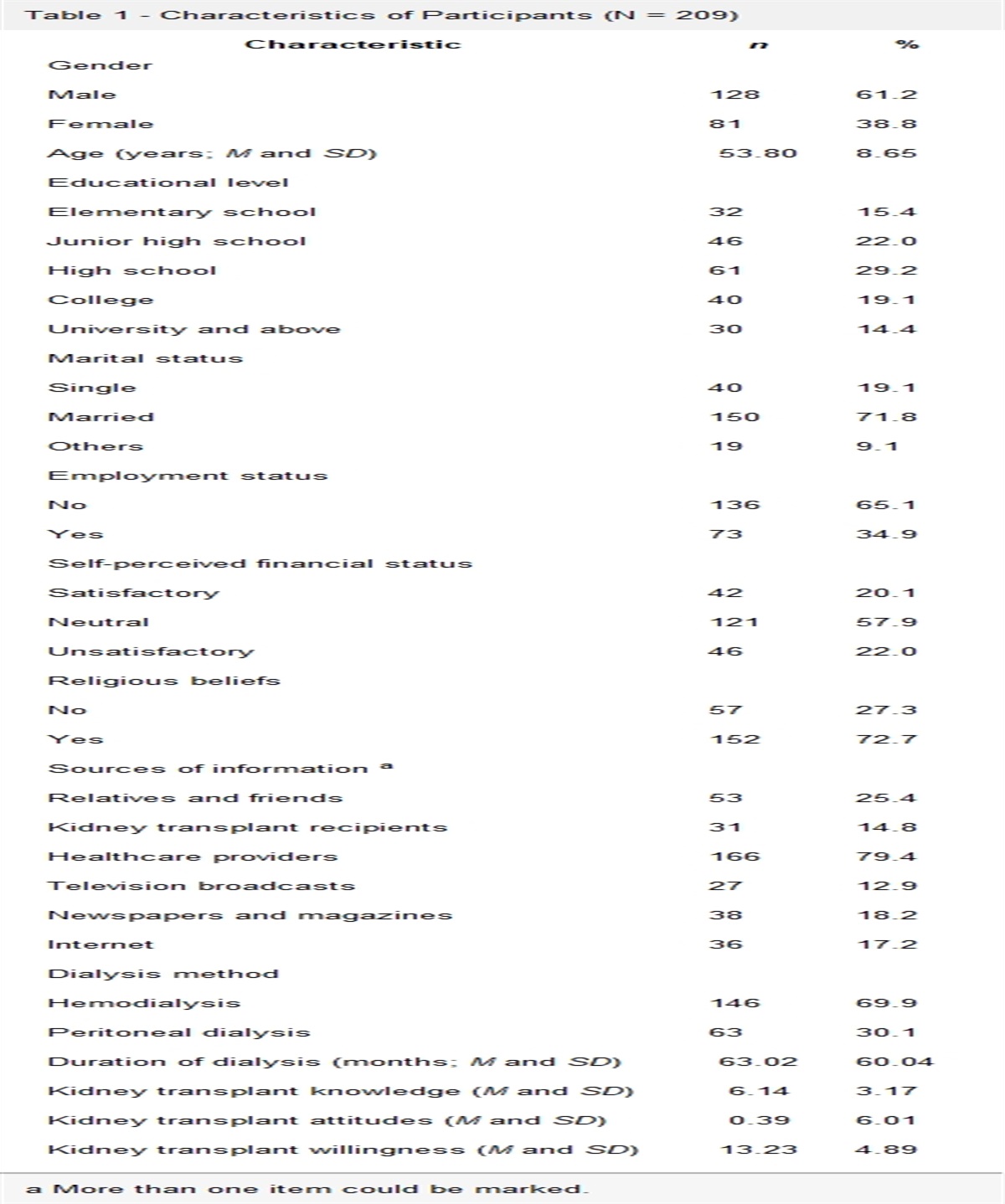
Results Sociodemographics and Disease HistoryMost (61.2%) of the participants were male, with ages ranging from 24 to 65 (mean = 53.80, SD = 8.65) years. The largest educational level category was high school (29.2%); most of the participants were married (71.8%) and unemployed (65.1%) and had religious beliefs (72.7%). Most perceived their financial status as adequate (57.9%). Most (79.4%) reported receiving information about KT from healthcare workers, and the average number of sources from which they had obtained information about kidney transplants was 1.68 (SD = 1.14), indicating participants' KT information sources were limited. Most (69.9%) had received hemodialysis, with dialysis durations ranging from 4 to 345 (mean = 63.02, SD = 60.04) months (Table 1). Thus, the average duration of dialysis of participants exceeded 5 years.
Table 1 - Characteristics of Participants (N = 209) Characteristic n % Gender Male 128 61.2 Female 81 38.8 Age (years; M and SD) 53.80 8.65 Educational level Elementary school 32 15.4 Junior high school 46 22.0 High school 61 29.2 College 40 19.1 University and above 30 14.4 Marital status Single 40 19.1 Married 150 71.8 Others 19 9.1 Employment status No 136 65.1 Yes 73 34.9 Self-perceived financial status Satisfactory 42 20.1 Neutral 121 57.9 Unsatisfactory 46 22.0 Religious beliefs No 57 27.3 Yes 152 72.7 Sources of information a Relatives and friends 53 25.4 Kidney transplant recipients 31 14.8 Healthcare providers 166 79.4 Television broadcasts 27 12.9 Newspapers and magazines 38 18.2 Internet 36 17.2 Dialysis method Hemodialysis 146 69.9 Peritoneal dialysis 63 30.1 Duration of dialysis (months; M and SD) 63.02 60.04 Kidney transplant knowledge (M and SD) 6.14 3.17 Kidney transplant attitudes (M and SD) 0.39 6.01 Kidney transplant willingness (M and SD) 13.23 4.89a More than one item could be marked.
Mean KT knowledge, attitude, and willingness scores were 6.14 ± 3.17, 0.39 ± 6.01, and 13.23 ± 4.89, respectively (Table 1), indicating participants had about 50% knowledge of KT, held neutral or slightly positive attitudes toward KT, and had 66% willingness to undergo a KT. In terms of KT willingness, 51.7%, 41.6%, 49.3%, and 50.2% agreed or strongly agreed that they would be willing to, respectively, register on a KT wait list, undergo deceased-donor KT, undergo live-donor KT, and undergo a KT.
Relationships Between Kidney Transplantation Willingness and Sociodemographics, Disease History, Knowledge, and AttitudesGender (t = 2.04, p = .043), age (r = −.26, p < .001), educational level [F(3, 205) = 4.38, p = .005], marital status (t = 2.49, p = .014), employment status (t = −3.65, p < .001), and dialysis duration (r = −.15, p = .036) were found to relate significantly to KT willingness. Specifically, being male, younger, single, and employed; having an education level of college or above; and having a shorter dialysis duration were associated with higher mean KT willingness scores. By contrast, self-perceived financial status, religious beliefs, information sources, and dialysis methods were not associated with KT willingness. Furthermore, KT knowledge and attitude scores correlated positively with KT willingness scores (r = .51 and r = .40, respectively; both ps < .001; Table 2). This indicates better knowledge of KT and more-positive attitudes are associated with greater willingness to undergo a KT.
Table 2 - Correlations Between Characteristics and Kidney Transplant Willingness (N = 209) Variable n Mean SD t/F/r p/Post Hoc a Gender 2.04 .043 Male 128 13.77 4.86 Female 81 12.37 4.83 Age (years) 209 −0.26 < .001 Educational level 4.38 .005 ① Elementary school 32 11.25 4.40 ④ > ① ② Junior high school 46 12.63 4.90 ③ High school 61 13.02 5.28 ④ College and above 70 14.71 4.37 Marital status 2.49 .014 Single 57 14.46 4.04 Married 152 12.77 5.10 Employment status −3.65 < .001 No 136 12.40 5.05 Yes 73 14.78 4.17 Self-perceived financial status 0.81 .445 Satisfactory 42 13.98 5.31 Neutral 121 13.19 4.83 Unsatisfactory 46 12.65 4.66 Religious beliefs 1.95 .053 No 57 14.30 4.88 Yes 152 12.83 4.84 Number of information sources 209 0.07 .294 Dialysis method −1.28 .201 Hemodialysis 146 12.95 4.76 Peritoneal dialysis 63 13.89 5.15 Duration of dialysis (months) 209 −0.15 .036 Kidney transplant knowledge 0.51 < .001 Kidney transplant attitudes 0.40 < .001Significant variables found in the univariate analysis (e.g., gender, age, dialysis duration, and KT knowledge and attitude scores) were incorporated into a multiple regression analysis to examine their power in terms of predicting KT willingness. The aforementioned variables together explained 45.4% of the variance in participants' KT willingness, F(10, 198) = 18.33, p < .001. Moreover, KT attitudes (β = .61, p < .001) and dialysis duration (β = −.11, p = .041) were identified as significant variables in the multiple regression analysis (Table 3).
Table 3 - Multiple Regression Analysis of Kidney Transplant Willingness (N = 209) Predictor B β t p Gender Female −.32 −.03 −0.06 .557 Male (ref.) Age −.06 −.10 −1.56 .119 Educational level Elementary school −.37 −.03 −0.41 .680 Junior high school .19 .02 0.25 .802 High school −.40 −.04 −0.60 .549 College and above (ref.) Marital status Married −.27 −.02 −0.43 .668 Single (ref.) Employment status Yes .47 .05 0.81 .417 No (ref.) Dialysis duration −.01 −.11 −2.06 .041 Kidney transplant knowledge .05 .04 0.57 .570 Kidney transplant attitudes .49 .61 10.22 < .001Note. R2 = .481, adjusted R2 = .454, F(10, 198) = 18.33, p < .001. Ref. = reference.
The mean KT willingness score in this study was 13.23 (out of 20), indicating a KT willingness of 66%, which is similar to the rates (50%–70%) previously reported in Western countries (Boima et al., 2021; Ilori et al., 2015; Kabbali et al., 2014). There are some reasons for this finding. First, KTs in Taiwan have become increasingly advanced and successful. Moreover, the Taiwan government has strongly advocated for KTs, and the cost of the procedure is covered under the National Health Insurance program. In addition, half (49.3%) of the participants either agreed or strongly agreed they would be willing to receive a live-donor KT. This is higher than the findings of previous research, in which only 16% of patients with ESRD in Taiwan were identified as willing to receive a live-donor KT (Chang, 2013). One reason for this discrepancy may be that Chang's study included participants over the age of 66 years. Older adults are generally less inclined to receive a KT (Alansari et al., 2017; Tan et al., 2017). Notably, 51.7% of the participants in this study either agreed or strongly agreed that they would like to register for a KT wait list. Healthcare professionals should educate KT candidates about KT preparations, preoperative evaluations, and KT procedures and prognosis to reduce patient anxiety. Moreover, shared decision-making may be useful in informing patients with chronic kidney disease about the impact of different decisions on renal replacement therapy as well as in improving decision-making self-efficacy and reducing decision-making conflicts (Ho et al., 2020). Furthermore, special attention should be focused on those who disagree or strongly disagree with registering for and accepting a KT to understand their problems and concerns and provide timely services.
This study found sociodemographics (e.g., gender, age, educational level, marital status, and employment) and disease history (e.g., dialysis duration) to be related to KT willingness. The average KT willingness score of male participants was higher than that of female participants, which is consistent with previous results (Calvo-Calvo et al., 2018; Kim et al., 2023). This disparity may relate to differences in the way men and women utilize healthcare services. Although women visit the doctor more often than men (You et al., 2019), men often utilize healthcare services in a business-like manner, are more likely to want active treatment, and may be more willing to undergo a major surgery (Reid et al., 2023). This study found younger participants to be relatively more willing to receive a KT, which is consistent with the findings of previous studies (Alansari et al., 2017; Tan et al., 2017). Possible reasons why older participants are less willing to undergo a KT are feeling comfortable with the status quo, lacking motivation to seek a transplant, and unwillingness to accept the related risks. The participants with an educational level of college or above were more willing to undergo a KT, which is also consistent with findings of previous studies (Alansari et al., 2017; Hamilton et al., 2017
Comments (0)