
Remember me



Patient safety incidents are a socially important health problem that not only threatens the lives of patients but also seriously affects the quality of healthcare services. Patients and family members may feel betrayed and seek revenge against healthcare professionals if, when patient safety incidents occur and healthcare institutions, healthcare providers fail to communicate appropriately (Y. Kim & Lee, 2021). After a patient safety incident occurs, patients and family members require healthcare providers to communicate with them about the incident and to minimize the damage caused by the incident (Y. Kim & Lee, 2021).
Disclosure of patient safety incidents refers to the process of discussing the causes and solutions of the incidents through effective communication with patients and family members (Choi et al., 2019). Disclosure is a system by which a medical institution voluntarily investigates the cause of patient safety incidents during medical practice, apologizes to the patient and family members, and provides appropriate compensation if a medical error is recognized (Moore & Mello, 2017). The process used to disclose patient safety incidents includes (a) providing an explicit statement that there has been an error, (b) describing what the error was, (c) explaining why the error happened, (d) explaining how prevention will be accomplished, and (e) offering an apology (Ok & Lee, 2017). Disclosure affects outcomes for patients and family members, the healthcare provider–patient relationship, healthcare providers (as secondary victims), and healthcare institutions (Hannawa et al., 2016). Therefore, disclosure of patient safety incidents is key to improving patient safety (Ok & Lee, 2017). Australia, Canada, the United States, and other countries have enacted regulations and guidelines related to the disclosure of patient safety incidents (Australian Commission on Safety and Quality in Health Care, 2020; Canadian Patient Safety Institute, 2011; Joint Commission Resources, 2022). However, no specific guidelines or legal protections for the disclosure of patient safety incidents are currently applied in Korea (Choi et al., 2019).
The effects of disclosing patient safety incidents are multifaceted. For patients and family members, filing medical litigation reduces the willingness to punish healthcare providers and increases the willingness to revisit, recommend, and trust healthcare providers or hospitals (Y. Kim & Lee, 2021). For medical staff, disclosure relieves guilt (Ock et al., 2017). Nevertheless, the fear of litigation or punishment due to the disclosure of patient safety incidents and the emotional distress of talking to patients about mistakes are obstacles to disclosure (Y. Kim & Lee, 2020c; Najafi Ghezeljeh et al., 2021). In Korea, although healthcare providers want to communicate transparently about patient safety incidents, there are no set guidelines or communication skills training available (Hannawa et al., 2016). Lack of training/education leads healthcare providers to be unprepared to discuss and disclose patient safety incidents (Dhamanti et al., 2023; Shapiro et al., 2021). Nurses who frequently interact with patients experience various patient safety incidents, leading them to experience difficulties such as stress and ethical conflicts during the disclosure of patient safety incidents (Y. Kim & Lee, 2020c).
Perceptions, attitudes, and competency with regard to overall patient safety, including the disclosure of patient safety incidents, are formed during nursing education (Y. Kim & Lee, 2020b). Therefore, education and interventions during nursing education that enhance the disclosure of patient safety incidents are required. According to the Knowledge, Attitude, and Practice model in the learning theory of education, positive attitudes, underscored by correct knowledge, regarding a certain desired behavior must be present for that behavior to occur (U.S. Agency for International Development, 2008). To identify the intervention effect, in this study, the following variables were selected based on this model: the knowledge of disclosure of patient safety incidents as the knowledge factor, the perception of disclosure of patient safety incidents and attitude toward patient safety as the attitude factor, and self-efficacy regarding disclosure of patient safety incidents as the practice factor.
Prior studies on the disclosure of patient safety incidents have been primarily qualitative or surveys, including reviews of patient safety incident disclosure (Ock et al., 2017), medical staff experiences with disclosure of patient safety incidents (Y. Kim & Lee, 2020c; Najafi Ghezeljeh et al., 2021), perceptions of disclosure of patient safety incidents (Y. Kim & Lee, 2020a, 2020b; Laoh, 2023), and experiences (Y. Kim & Lee, 2021) and attitudes (Ock et al., 2020) of patients and family members regarding the disclosure of patient safety incidents. Also, the attitudes and confidence of medical interns and fourth-year medical students toward patient safety incident disclosure were measured after a related training intervention (C. W. Kim et al., 2017). However, studies on the effect of education on knowledge and perception of disclosure of patient safety incidents, attitudes toward patient safety, and self-efficacy regarding the disclosure of patient safety among nursing students are lacking. Therefore, this study was designed to investigate the effect of a patient safety incident disclosure education program on the knowledge and perception of disclosure, attitudes toward patient safety, and disclosure self-efficacy of fourth-year nursing students.
HypothesesThe hypotheses of this study are as follows.
Hypothesis 1: Knowledge regarding patient safety incident disclosure will be higher in the experimental group than the control group. Hypothesis 2: Perception regarding patient safety incident disclosure will be more positive in the experimental group than the control group. Hypothesis 3: Attitudes toward patient safety incident disclosure will be more positive in the experimental group than the control group. Hypothesis 4: Self-efficacy regarding patient safety incident disclosure will be higher in the experimental group than the control group. Methods Design and ParticipantsThis quasi-experimental study used a nonequivalence control group pretest–posttest design.
Design and ParticipantsThe participants were fourth-year undergraduate students enrolled in the nursing departments of Hanyang University in Seoul City and Kyungpook National University in Daegu City. The total number of participants was 55 in the experimental group and 114 in the control group. The two universities follow the same standard Korean nursing education curriculum and operate the same nursing management course, which is mainly designed to teach patient safety, during the first semester of the fourth year. The participants were recruited on a first-come, first-served basis. Participation was voluntary, and all participants gave written informed consent to participate. Fourth-year nursing students were targeted in this study because they had already been taught the basic concepts of patient safety in courses on fundamental nursing and nursing management. In addition, nurses in Korea must take an active role in ensuring patient safety and disclosing patient safety incidents within 1 year of graduation after entering the medical system (Jang, 2018).
Hanyang University students were assigned to the experimental group, and Kyungpook National University students were assigned to the control group to prevent intergroup contamination. The recruitment notice was posted on the universities' student bulletin boards and on social network sites. An explanation of the study was provided via email or social networking service to students who contacted the researcher. A link to the participation guide and study details was provided to those who wished to participate, and consent was obtained before participation.
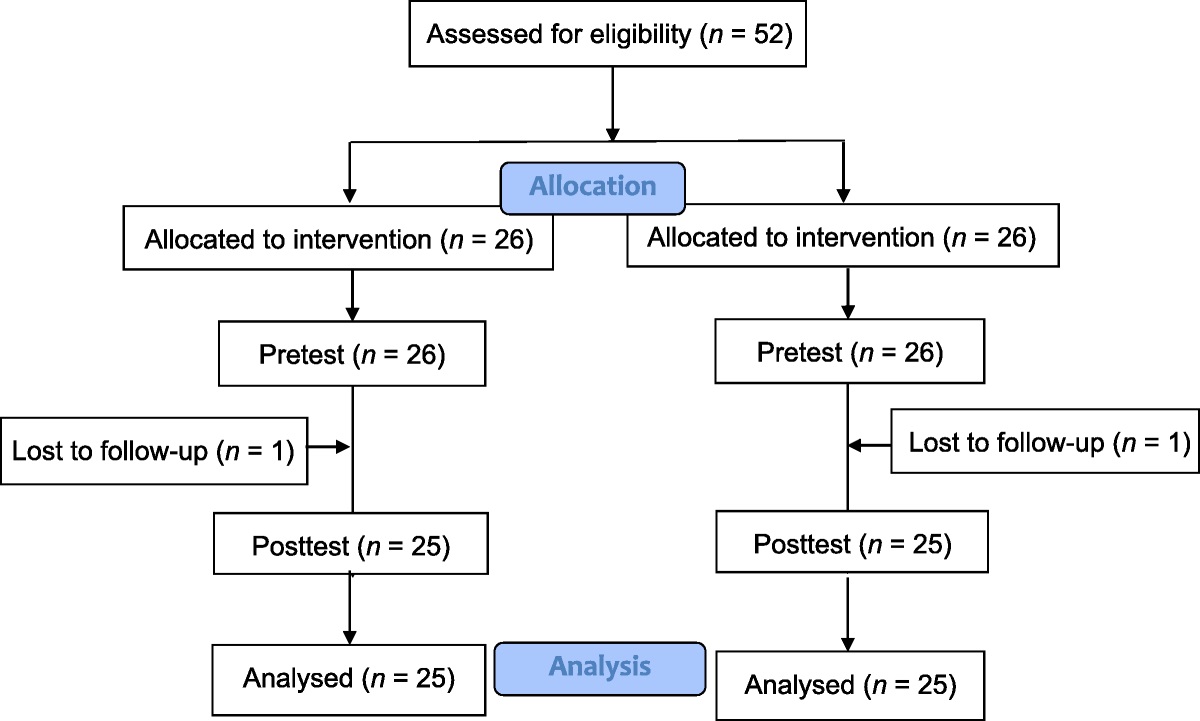
The number of participants required for the study was calculated using G*Power Version 3.1.9. A minimum of 42 participants with 21 participants per group was calculated based on effect size = 0.90, power = 0.80, and significance level = .05. Regarding the effect size, as no previous studies have examined disclosure programs for patient safety incidents targeting nursing students, this study referenced the investigation of Mok and Kim (2020) of a patient safety communication education program. After accounting for potential withdrawals, 52 participants were enrolled in this study, including 26 in the experimental group and 26 in the control group. One person withdrew from each group (dropout rate of 3.8%), leaving the data from 50 participants available for analysis (Figure 1).
 Figure 1:
Figure 1: Flow Diagram
Instruments General characteristicsGeneral characteristics of the participants, including age, gender, satisfaction with nursing major, satisfaction with clinical practice, experience receiving undergraduate patient safety education, experience witnessing patient safety events related to medical staff during clinical practice, and direct experience with patient safety events related to themselves during clinical practice, were investigated.
Knowledge of disclosure of patient safety incidentsThe knowledge of disclosure of patient safety incidents questionnaire developed by the researcher was utilized. This instrument covers knowledge of the concept and method of disclosure of patient safety incidents, standards to be implemented, positive effects, obstacles, and implementation methods. The content validity index score for this questionnaire, validated by three nursing professors, was .89. The questionnaire includes six questions scored on a 4-point Likert scale (1 = I don't know at all, 4 = I mostly know). The total score is calculated as the average of all item scores and ranges from 1 to 4. In this study, the Kuder–Richardson Formula 20 was .899.
Perception of disclosure of patient safety incidentsThe perception of open disclosure of patient safety incidents among nurses scale developed by Y. Kim and Lee (2020a) was used in this study to measure perception of disclosure of patient safety incidents. This tool comprises 30 questions in the following six domains: open disclosure across harm level (three questions), open disclosure across situations (six questions), justification of open disclosure (four questions), negative consequences of open disclosure (five questions), positive consequences of open disclosure (six questions), and facilitators of open disclosure (six questions). Answers are rated on a 4-point Likert scale (1 = completely disagree, 4 = completely agree). The total score is calculated as the average of all item scores and ranges from 1 to 4, with higher scores indicating a more positive perception of patient safety incident disclosure. The reliability of this measure was Cronbach's α = .895 at the time of development and was .814 in this study.
Attitudes toward patient safetyAttitudes toward patient safety were measured using a tool initially developed by Madigosky et al. (2006) for medical students and subsequently modified by Hyeon (2015). This tool consists of 13 questions related to patient safety incident reporting, importance of patient safety, and response in the event of patient safety incidents. Answers are rated on a 5-point Likert scale (1 = not at all, 5 = strongly agree). The total score is calculated as the average of all item scores and ranges from 1 to 5, with higher scores indicating more positive attitudes toward patient safety. The reliability of this measure was Cronbach's α = .62 at the time of development and was .58 in this study.
Self-efficacy regarding disclosure of patient safety incidentsSelf-efficacy regarding disclosure of patient safety incidents was measured using the following item developed by the researcher: “I am confident in communicating adverse events to patients.” The content validity index of this measure, as validated by three nursing professors, was 1.0. Answers were rated on a 5-point Likert scale (1 = not at all, 5 = strongly agree). The total score ranges from 1 to 5, with higher scores indicating higher self-efficacy.
Study Procedure PrescreeningThe researcher conducted prescreening using the online questionnaires directly for fourth-year nursing students who had submitted their written consent. The general characteristics of the experimental and control groups with regard to knowledge and perceptions of patient safety incident disclosure, attitudes toward patient safety, and self-efficacy regarding the disclosure of patient safety incidents were investigated. The estimated time required to complete the questionnaire was 15 minutes.
Study methodThe researcher reviewed previous studies and guidelines related to the disclosure of patient safety incidents to develop the patient safety incident disclosure education program used in this study. Program composition and contents were developed based on previous studies, which had used interviews with nurses (Y. Kim & Lee, 2020c), interviews with patients and family members (Y. Kim & Lee, 2021), and research into the perceptions of nurses and nursing students regarding the disclosure of patient safety incidents (Y. Kim & Lee, 2020a, 2020b). The developed education program was reviewed by two professors from the college of nursing who are experts in the field of patient safety and have directly performed patient safety tasks in medical institutions.
The program was conducted online using a learning management system by the researcher for the experimental group between September 6 and October 22, 2021. Six groups of four to five people each were formed, with each group participating in the program for 5 days. The eight modules of the program included orientation and overview of patient safety, disclosure of patient safety incidents and effects, obstacles to disclosing patient safety incidents, methods of disclosing patient safety incidents, examples, guidelines, activation strategies, and Case Studies 1–3 as well as a course evaluation. After modules were grouped according to content, Module 1 was conducted on Day 1, Modules 2–7 were conducted on Days 2–4 (two modules per day), and Module 8 was conducted on Day 5 (Table 1).
Table 1 - Patient Safety Incident Disclosure Education Program for Undergraduate Nursing Students Day Module Contents TimeNote. DPSI = disclosure of patient safety incidents.
Educational methods, videos, lectures, case activities, discussions, quizzes, and reflections produced by the researcher were used, and each module lasted for 90–120 minutes. Three virtual cases of patient safety events corresponding, respectively, to red light events, adverse events, and proximity errors were presented after watching lectures or videos. Subsequently, opinions were discussed within the group by preparing a case activity report on whether disclosure of patient safety incidents should be made and what to do when disclosing safety incidents. A three- to five-question quiz was administered to assess the content learned. The control group had the option to participate in the developed program after the postscreening and intervention program had been completed.
PostscreeningPostscreening was conducted on Day 5 for both groups using an online survey.
Ethical ConsiderationsThis study was conducted after approval had been received (No. KNU-2021-0142) from the institutional review board of the university. Written informed consent was obtained from all of the participants, and their anonymity was guaranteed. The data collected during participation were used for research purposes only, and participants could withdraw at any time with no consequences. After the completion of the postscreening survey, a gift was provided to all of the participants to show appreciation.
Data AnalysisThe collected data were analyzed using IBM SPSS Statistics 25.0 (IBM Inc., Armonk, NY, USA). The general characteristics data and values for each variable were analyzed using descriptive analysis. Normality tests for the experimental and control groups were performed using the Kolmogorov–Smirnov normality test. Homogeneity between the two groups was analyzed using the t test, χ2 test, Fisher's exact test, and Mann–Whitney U test. To test the hypotheses, the main variables of the experimental group and control groups were analyzed using the t test, Mann–Whitney U test, and Wilcoxon signed-rank test. Before the intervention, as knowledge on patient safety incident disclosure was not homogeneous between the groups, ranked analysis of covariance was used for analysis. The effect sizes were calculated using Cohen's d statistic.
Results Homogeneity Test for Participant Characteristics and VariablesThe homogeneity of general characteristics and of the knowledge, perception, and self-efficacy regarding patient safety incident disclosure between the experimental and control groups were analyzed before implementing the education program. There were no significant differences between the two groups in terms of perception, attitudes, and self-efficacy, suggesting the two groups to be homogeneous. However, knowledge related to the disclosure of patient safety incidents was significantly higher in the control group (2.65) than the experimental group (2.30; Table 2).
Table 2 - Homogeneity Test of General Characteristics and Dependent Variables Between the Experimental and Control Groups (N = 50) Characteristic Experimental Group (n = 25) Control Group (n = 25) χ2/t/z p n % n % Age (years; M and SD) 22.68 1.55 22.80 1.44 −0.42 .676 Gender 2.45 .118 Male 4 16.0 0 0 Female 21 84.0 25 100 Satisfaction with major (M and SD) 3.80 0.76 3.60 0.87 −0.77 .442 Satisfaction with clinical practice (M and SD) 3.64 0.70 3.36 0.81 −1.01 .313 Patient safety education experience 0.00 < .999 No 3 12.0 3 12.0 Yes 22 88.0 22 88.0 Witnessing patient safety incidents during clinical practice 0.75 .387 No 12 48.0 8 32.0 Yes 13 52.0 17 68.0 Direct experience of patient safety incidents during clinical practice 1.71 .192 No 24 96.0 20 80.0 Yes 1 4.0 5 20.0 Knowledge of DPSI (M and SD) 2.30 0.46 2.65 0.44 2.78 .008 Perception of DPSI (M and SD) 3.26 0.28 3.21 0.24 −0.71 .484 Attitude toward patient safety (M and SD) 4.13 0.30 4.04 0.34 −1.02 .315 Self-efficacy regarding DPSI (M and SD) 3.12 0.83 3.28 1.10 −0.66 .510Note. DPSI = disclosure of patient safety incidents.
Because knowledge related to patient safety incident disclosure was not homogeneous between the groups, covariance analysis was performed using the knowledge before intervention as a covariate (Table 3). Patient safety incident disclosure knowledge increased by 1.07 (from 2.30 pretest to 3.37 posttest) in the experimental group and by 0.19 (from 2.65 pretest to 2.84 posttest) in the control group, showing a statistically significant difference between the groups (t = −6.23, p < .001). The Cohen's d effect size was 1.76 with large effects observed (Cohen, 1988). Thus, the first hypothesis was supported.
Table 3 - Differences in Dependent Variables Between the Experimental and Control Groups (N = 50) Variable Experimental GroupNote. DPSI = disclosure of patient safety incidents.
a Within group. b Between group.
Perception of patient safety incident disclosure increased by 0.17 (from 3.26 pretest to 3.43 posttest) in the experimental group and by 0.03 (from 3.21 pretest to 3.24 posttest) in the control group, showing a statistically significant difference between the groups (t = −2.22, p = .031). The Cohen's d effect size was 0.63 with medium effects observed (Cohen, 1988). Thus, the second hypothesis was supported.
Attitudes toward patient safety decreased by −0.03 (from 4.13 pretest to 4.10 posttest) in the experimental group and by −0.02 (from 4.04 pretest to 4.02 posttest) in the control group, revealing no significant difference between the groups (t = 0.12, p = .908). The Cohen's d effect size was 0.03 with small effects observed (Cohen, 1988). Thus, the third hypothesis was rejected.
Self-efficacy regarding patient safety incident disclosure increased by 1.08 (from 3.12 pretest to 4.20 posttest) in the experimental group and decreased by −0.12 (from 3.28 pretest to 3.16 posttest) in the control group, showing a significant difference between the groups (z = −4.36, p < .001). The Cohen's d effect size was 1.23 with large effects observed (Cohen, 1988). Thus, the fourth hypothesis was supported.
DiscussionIn this study, a patient safety incident disclosure education program for nursing students was evaluated in terms of its effects on related knowledge and perceptions, attitudes toward patient safety, and self-efficacy regarding patient safety incident disclosure. The key findings are discussed in this section.
First, the program improved knowledge of disclosure of patient safety incidents. These results were consistent with previous studies in which patient safety knowledge scores increased after patient safety education was provided to nursing students (e.g., Maxwell & Wright, 2016; Park & Kim, 2016). In this study, knowledge of disclosure of patient safety incidents before the program was low, with an average score of 2.30 out of a total possible 4 for the experimental group and 2.65 for the control group. A prior survey on patient safety education conducted on fourth-year students at a nursing university in Korea found that most students had been taught about patient safety only in the context of falls, medications, infections, bedsores, and safety accidents (Park & Kim, 2016). This suggests that knowledge regarding disclosure of patient safety incidents is not sufficiently emphasized in the Korean nursing education curriculum. In the training program in this study, eight modules for disclosure of patient safety incidents were implemented for a total of 570 minutes. Through this program, knowledge of disclosure of patient safety incidents improved through systematic learning from the basic concept of disclosure of patient safety incidents to guidelines and case studies. In addition, the participants were encouraged to think and reflect on cases by implementing case activities and discussion rather than being provided knowledge only. However, this study was limited in terms of the effect of education on knowledge being indirectly measured through a self-report questionnaire.
The program also significantly improved participant perceptions of patient safety incident disclosure. The average posttest perception score of 3.43 for the experimental group was significantly higher than the average score of 3.03 found in a previous study (Y. Kim & Lee, 2020a) that used the same instrument. In previous studies, nurse perceptions regarding patient safety incident disclosure were found to be relatively low due to an immature patient safety culture in medical institutions and the lack of a disclosure support system (Y. Kim & Lee, 2020a). One prior study in which data were collected by interviewing intensive care unit nurses reported that nurses found it difficult to communicate patient safety incidents due to fear of punishment or stigma (Najafi Ghezeljeh et al., 2021). Thus, disclosure regulations on patient safety incidents should be enacted in Korea that prevent nurses from being disadvantaged due to disclosure and ensure consolations and apologies provided by medical personnel may not be used as evidence of legal liability (Lee et al., 2017). These legal and institutional devices are necessary to establish a positive patient safety culture in medical institutions and allow medical personnel to perceive patient safety incident disclosure positively and implement this mechanism when appropriate.
Moreover, this program was found to improve patient safety incident disclosure self-efficacy. In prior studies, nurses were found to lack the confidence necessary for effective related communications due to the lack of directives, guidelines, or education on how to communicate with patients and family members regarding patient safety incidents (Y. Kim & Lee, 2020a; Shapiro et al., 2021). Therefore, to develop the capacity for disclosure of patient safety incidents, it is necessary to educate nurses on the importance and methods of patient safety incident communication during their undergraduate education. In addition to the basic concepts and importance of patient safety, this education should focus on fostering interpersonal relationship and communication skills, nursing ethics, and patient-centered thinking. Integrating this program in the upper-grade
Comments (0)