
Remember me



Collaboration and coordination among medical team members play a pivotal role in delivering high-quality medical care. The World Health Organization (WHO, 2016) recognizes the crucial role of nurses and midwives, who account for nearly 50% of the global health workforce. As frontline caregivers, their initial assessment, care, and treatment significantly influence patient outcomes. Regularly assessing the clinical competency of nurses is essential to maintaining the quality of health service provision. Furthermore, head nurses have the potential to inspire and motivate their staff and thus to elevate the competency of nurses (Y. J. Kim et al., 2011). Therefore, evaluating the relationship between the clinical competence of nurses and various factors, particularly head nurse leadership style, is important. Insights into the influences of staff nurse demographics and head nurse leadership style on clinical competency may guide and help healthcare providers develop more effective strategies for enhancing patient care and fostering a positive work environment. In light of these considerations, this study was developed to investigate the relationship between the leadership style of head nurses, clinical competence in staff nurses, and other relevant demographics. The goal of this study was twofold: (a) systematically assess the currently uncertain role of head nurse leadership in staff nurse clinical competency and (b) suggest improved training practices that leverage this relationship to improve nursing care competency. In light of the important role nurses play in patient care, shedding light on this little-explored nexus is crucial to unlocking the full potential of staff nurses.
A literature review conducted to identify the potential variables for this study revealed four areas for consideration: (a) leadership and leadership style, (b) nursing clinical competency, (c) established links between the staff nurse characteristics and clinical competency, and (d) established links between head nurse leadership style and staff nurse clinical competency.
Leadership and Leadership StylesA leader inspires and guides followers to achieve a specific objective (Nawaz et al., 2016; Valiga, 2019). In essence, leadership is the cornerstone of an organization's success, as it illuminates the vision and drives maximum results (Nawaz et al., 2016). Leadership involves influencing others to attain their fullest potential regardless of the task or project. It is important to note that leadership and management are two distinct skill sets. A leader focuses on people and develops strategies to drive growth, whereas a manager prioritizes systems and structure and administers day-to-day operations (Valiga, 2019). Ultimately, leadership and management are complementary, as strong relationships are key to effective leadership and are facilitated by management practices (Valiga, 2019).
Over time, leadership theories have evolved and adapted to changing cultural and societal norms, resulting in varying assumptions, focuses, causal links, lenses, values, terminology, and perspectives (Specchia et al., 2021). In the early days, researchers were mainly interested in identifying the innate personality traits that distinguish successful leaders from nonleaders (Nawaz et al., 2016). Another prevalent theory suggests that leaders who adopted democratic or participative styles are more successful (Balbuena et al., 2020; Nawaz et al., 2016). More recently, situational deliberations have also been considered to determine leaders' success; those who could understand contextual issues and choose the appropriate management style for each circumstance tend to be more effective (Balbuena et al., 2020).
Bass (1985) defined two contrasting leadership styles: transactional and transformational. Transactional leaders are instrumental and focus on exchanging relationships with their team members, whereas transformational leaders are visionary and enthusiastic, with an inherent ability to motivate members (Bass, 1985). Transformational leadership promotes trust and highlights higher levels of interdependence between the leader and members. Conversely, transactional leadership uses traditional values to establish a team's objective and a transparent reward system based on the performance partnership of team members (Bass, 1985). Transformational and transactional leadership styles, rather than being exclusive concepts, should be seen as a continuum influenced by similar sets of factors (Judge & Piccolo, 2004). Leaders usually combine transformational and transactional leadership styles when leading their teams rather than focusing on one style (Bass, 1985).
Nursing Clinical CompetencyCompetency is a construct that describes an individual's ability to perform a job. In the context of nursing, competency directly impacts job performance and organizational success (Savanevičienė et al., 2008). For nurses, clinical competency leads to improved patient care quality, higher patient satisfaction with nurses, and greater respect for the nursing profession as a whole (Karaca & Durna, 2019). The WHO provides policies and strategies for member countries to help strengthen professional competency in nurses (WHO, 2016, 2021).
Several models, including behaviorism, trait theory, and holism, have been proposed to explain nursing clinical competency (Nabizadeh-Gharghozar et al., 2021). Behaviorism emphasizes the ability to perform core skills; trait theory considers the individual traits (e.g., knowledge and critical thinking skills) necessary for effective duty performance (Fukada, 2018); and holism considers the professional knowledge, skills, attitudes, and personal abilities required of nurses in clinical settings (Takase & Teraoka, 2011).
Staff Nurse Characteristics and Clinical CompetencyClinical competency encompasses the wide range of skills, knowledge, attitudes, values, and abilities necessary for effective professional performance (Fukada, 2018; Levett-Jones et al., 2011). This multidimensional concept is influenced by a variety of demographic, work environment, management, and other factors (Fukada, 2018). For example, length of employment (Currie, 1994; Takase, 2013; Yamamoto et al., 2021), department (Yamamoto et al., 2021), and the ease of getting days off (Yamamoto et al., 2021) have previously been found to affect clinical competency. Also, clinical competency was found to be significantly higher in nurses in South Korea who were over 31 years old and married and with more than 15 years of employment experience (Y. J. Kim et al., 2011).
In addition, clinical competency has been shown to differ significantly based on age, marital status, level of education, current working department, and clinical experience in South Korea (S. O. Kim & Choi, 2019). Similarly, evidence-based practice competency was found to be higher among nurses who were 36 years or older, married, and educated to the graduate school level and possessed over a decade of work experience, with no effect on competency found for either job position or work department (Lee et al., 2020). Personal characteristics such as a clear vision of goals and strong interpersonal relationships may also impact clinical competency (Yamamoto et al., 2021). These findings further emphasize the importance of understanding the multifaceted nature of clinical competency and the various factors that impact this concept in different contexts.
Leadership Style and Staff Nurse Clinical CompetencyThe relationship between leadership and performance has been extensively studied, especially in terms of the influence of leadership style. It is important to note that performance is not the same as competency. Although leadership style may greatly impact organizational and employee performance, many factors, including competency, contribute to job performance (Kolibáčová, 2014; Tzeng, 2004). In addition, transformational leadership has been shown to increase employee performance (Baig et al., 2021).
In nursing, leadership style has been linked to stress, turnover intention, and job satisfaction in staff nurses (Labrague et al., 2020; Pishgooie et al., 2019; Specchia et al., 2021). Thus, transforming leadership is considered a critical element in transforming healthcare systems (Institute of Medicine, 2011). Beyond organization and delegation skills, nursing leadership involves leveraging interpersonal skills to help team members reach their full potential (Pullen, 2016). As first-line managers, head nurses are responsible for creating stable work environments that foster a sense of belonging and allow team members to demonstrate professional competence (Lu et al., 2002).
Few studies have explored the relationship between the leadership styles of head nurses and clinical competency in their staff nurses. The qualitative study of Purfarzad et al. (2019) identified leadership as playing a supportive role in competency development. In South Korea, Lee et al. (2020) employed multiple regression analysis and determined critical thinking disposition and transformational leadership to be the most influential factors affecting staff nurse competency in evidence-based practice. Chang (2008) explored the influence of Chinese cultural values on nursing leadership styles in Taiwan using multivariate analysis of variance (MANCOVA), finding a significantly positive association between cultural values and perceptions of leadership behavior.
Most related studies in the literature have focused on elucidating the relationship between leadership style and performance. Thus, a significant knowledge gap remains with regard to the influence of nurse demographics on their clinical competency as well as the interplay between head nurse leadership style and staff nurse clinical proficiency. Therefore, this research was designed to help bridge these gaps by exploring the impact of staff nurse demographics on clinical competency as well as the correlation between the leadership style of head nurses and staff nurse clinical competency. Furthermore, the effect of key demographic variables on staff nurse clinical competency after controlling for the influence of head nurse leadership was investigated. Based on the above aims, the following four research questions (RQs) were posited:
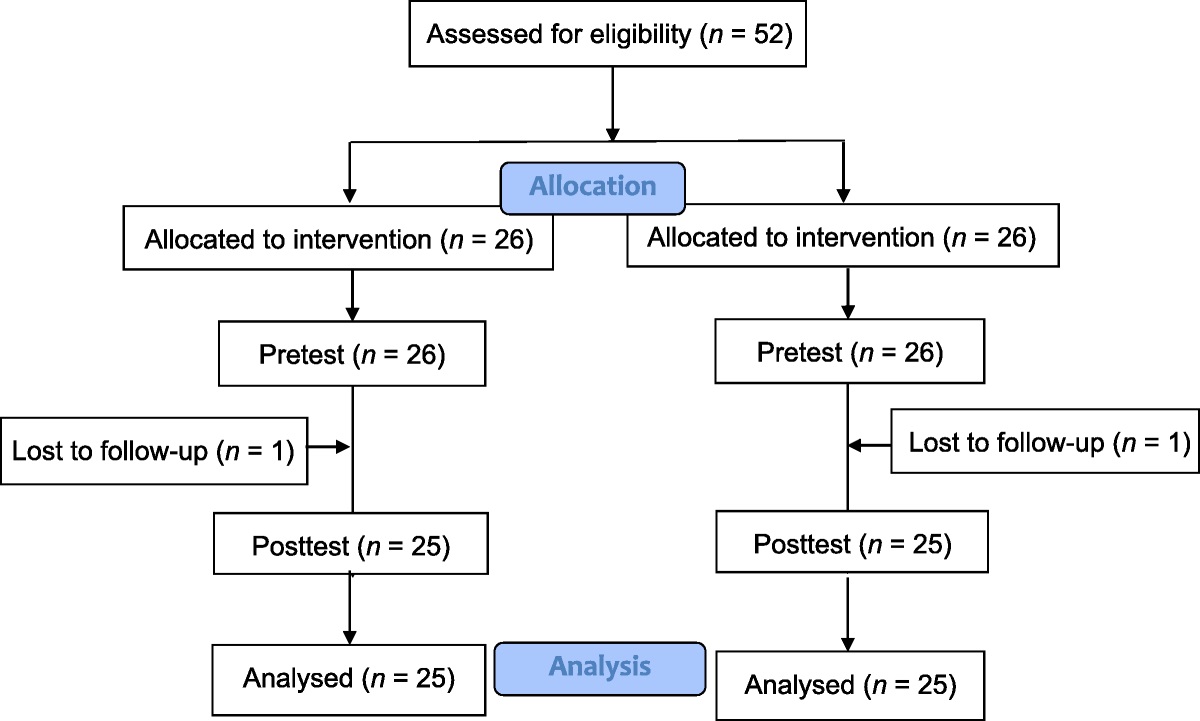
RQ1: Which head nurse leadership styles, staff nurse demographics, and staff nurse clinical competencies should be considered? RQ2: How do demographic variables influence self-perceived clinical competency among staff nurses? RQ3: Does a significant correlation exist between head nurse leadership style and staff nurse clinical competency? RQ4: What are the effects of the identified demographic variables (i.e., gender, age, marital status, educational level, job title, employment department, length of employment) on staff nurse clinical competence after controlling for head nurse leadership style? Methods ProcedureCluster sampling was used in this cross-sectional study to recruit staff nurses from a national medical center in northern Taiwan. After receiving approval from the institutional review board, participants were recruited between 2017 and 2018. Bedside nurses working in their current ward for at least 1 year were invited to participate. One-stage random cluster sampling was employed, with all nurses in a randomly selected ward sampled and invited to participate. Each ward was considered as a single cluster and assigned a number from 1 to 89, from which 20 were selected based on random numbers generated by a computer.
Participation was voluntary and anonymous. The researcher explained the purpose of the study to all of the 379 eligible participants via a written research statement. This statement did not request the participants' identifying information. Upon obtaining verbal consent, one researcher delivered the printed survey in an opaque envelope. The researcher returned to the participating wards weekly over a 6-month period to retrieve the completed surveys sealed in the provided envelope from the collection box.
A priori power analysis was conducted using G*Power Version 3.1.9.7 (Faul et al., 2009) to determine the minimum sample size with 80% power for a medium effect at a significance criterion of α = .05 (Cohen, 1992). The input parameters were as follows: (1) test family for RQ2 is F test, that for RQ3 is exact test, and that for RQ4 is F test; (2) statistical test for RQ2 is ANOVA (fixed effects, omnibus, one-way), that for RQ3 is correction-bivariate normal model two-tailed tests, and that for RQ4 is MANCOVA (global effects); (3) medium effect size was f = 0.25 in RQ2, r = .3 in RQ3, and f2 = 0.150 in RQ4; and (4) the number of groups in RQ2 was four in age, two in marital status, three in educational level, three in job title, and three in the length of employment, whereas the number of groups in RQ4 was 16. The required sample size for the RQ2 ANOVA test was 159. However, to account for the nonparametric test, the number was increased to 183 after adding a 15% buffer (Lehmann, 2006). The required sample sizes for RQ3 and RQ4 were 84 and 144, respectively. After adding an additional 35% for potential attrition, the estimated sample size required for this study was determined as 195.
MeasuresThe paper survey administered to the participants comprised three measures: a demographic questionnaire, the Multifactor Leadership Questionnaire (MLQ) in traditional Chinese (Wu & Lin, 1998), and the Clinical Competency Scale (CCS) in traditional Chinese (Wang et al., 2011). The demographic questionnaire collected information on gender, age, marital status, level of education, job title, employment department, and length of employment.
Multifactor leadership questionnaireThe MLQ (Bass & Avolio, 1990), designed to assess two leadership styles (i.e., transformational and transactional), has been widely used in many fields and in more than 30 countries (Boamah & Tremblay, 2019) and has been translated from the original English into many other languages. The traditional Chinese version (Wu & Lin, 1998) of the original MLQ (Bass & Avolio, 1990) used in this study includes 65 questions that are scored on a 5-point Likert scale (0–4) and has a Cronbach's alpha of .85–.97. Higher scores indicate stronger leadership skills. For this study, two terms on this scale were updated to reflect current nursing management usage. “Supervisor” was rephrased to read “head nurse,” and “subordinate” was rephrased to read “staff nurse.” Because only these two nouns were updated, the validity and reliability of the scale were not affected.
Clinical competency scaleThe CCS was modified based on Wang et al. (2011) in traditional Chinese. The CCS includes 75 questions on a 5-point Likert scale (0–4) with five components: patient care (ability to assess health issues and apply evidence-based practice, create an appropriate nursing plan, provide individualized nursing intervention, and evaluate outcomes effectively), professionalism (integrality with ethical and professional disposition), knowledge (active participation in continuous education, mentoring peers and supervising student nurses, assisting or supporting the nursing project or research), communication skills (effectively collaborating with a professional team, establishing therapeutic rapport with patients and family, responding timely and clearly), and management (modeling the high-quality nursing service provider, effective conflict resolution and nursing management). Higher scale scores indicate higher levels of clinical competency. The original scale had a Cronbach's alpha of .97. To fit better with the nursing context, we modified two traditional Chinese characters (words) in the original scale. The modified CCS had a Cronbach's alpha of .88–.95 (patient care = .90, professionalism = .88, communication skills = .89, management = .95, and knowledge = .94).
Ethical ConsiderationsThe first author's institutional review board approved the study (TPEVGH IRB No. 2016-08-027 BC), and the study was implemented in consultation with the research site. Staff nurse participation was voluntary, and no monetary incentive was offered. No identifying information was collected, and the study used a written research statement with verbal consent. All participants received a gift of a water bottle valued at US$8.00.
Data AnalysisIBM SPSS Statistics for Windows Version 27.0 (IBM, Inc., Armonk, NY, USA) was used for descriptive and inferential statistics. The distributions of demographic variables were unequal across the samples, and some samples had less than 30 participants. Before conducting inferential statistics, the Kolmogorov–Smirnov test was applied to examine whether the demographic variables were normally distributed. The results for all of the demographic variables indicated abnormal distribution (p < .001).
To address the second RQ, nonparametric analysis (i.e., Mann–Whitney U and Kruskal–Wallis) was used due to abnormality. The Mann–Whitney U test was used to analyze gender and marital status, and the Kruskal–Wallis test was used to examine age, educational level, job title, employment department, and length of employment. In addition, the Bonferroni correction was used for the Kruskal–Wallis test.
To address the third RQ, Spearman's rank correlation coefficient was used to examine the relationship between head nurse leadership style and staff nurse clinical competency.
To address the fourth RQ, a series of exploratory analyses of covariances (ANCOVAs) were initially performed using transformational leadership as a covariate to control its effect on clinical competency. Due to the sharply unequal cell sizes for educational level and job title, the authors removed these from the ANCOVA and subsequent analyses. As age and length of employment were found to be strongly related (r = .98, p < .001), age was removed as a variable, and length of employment was retained as a more meaningful variable for exploring staff nurse competency. Marital status was found to be an insignificant factor and was dropped from subsequent analyses. Assumptions were met. Levene's test was not significant, F(2, 165) = 0.74, p = .48. Finally, ANCOVA was used to determine the influence of length of employment on clinical competency after controlling for the transformational leadership style. Transformational leadership was identified as a significant predictor of clinical competency, whereas transactional leadership was not. Composite scores for clinical competency were used for length of employment, F(2, 144) = 11.50, p < .001, η2p = .14, with the effect sizes found to be large. The results for the exploratory ANCOVA are shown in Table 4.
After the exploratory ANCOVAs and after controlling for head nurse leadership style, the effect of employment length on each clinical competency component was explored using MANCOVA.
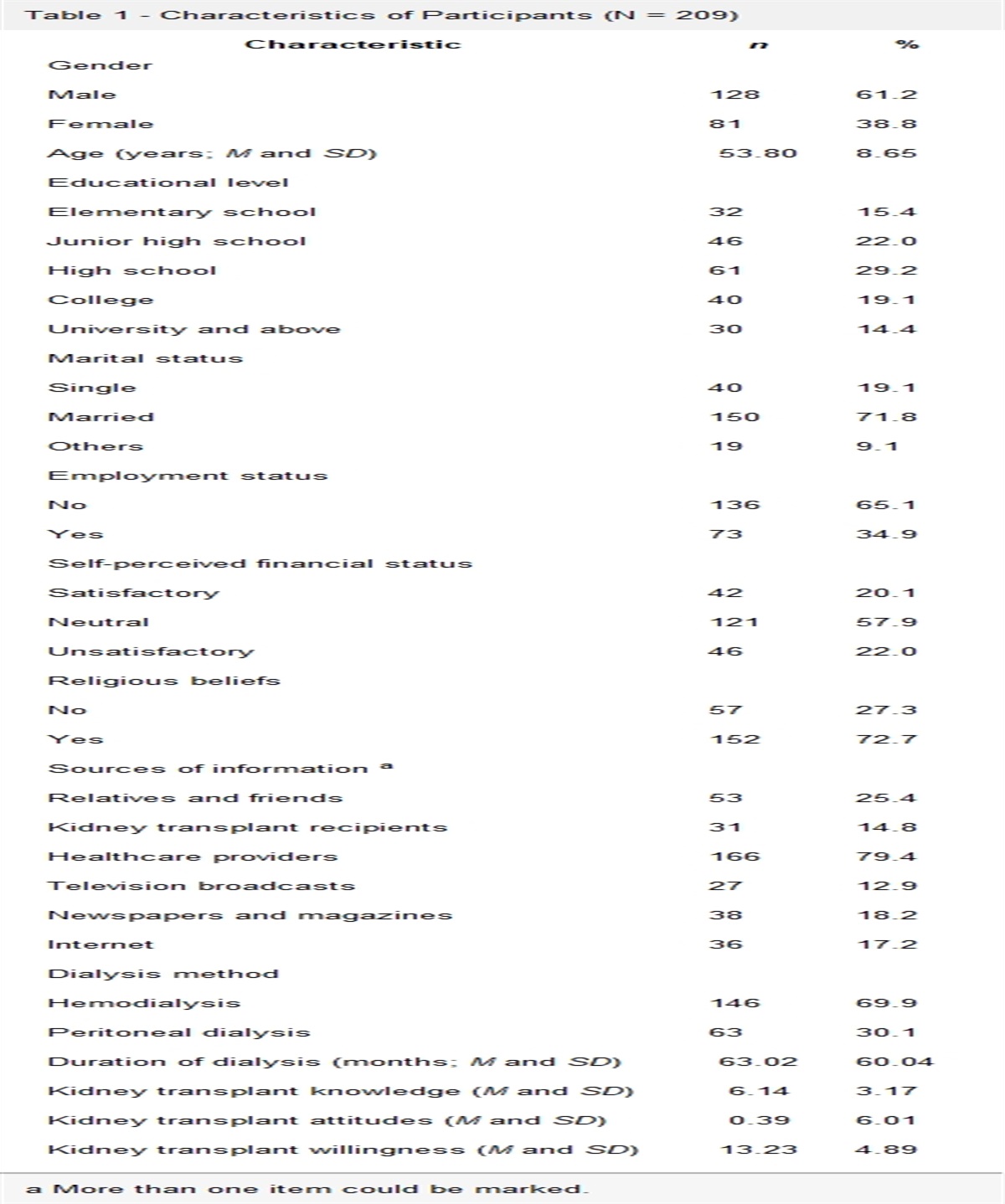
ResultsThis study invited 379 students to participate, with 200 returning the completed survey (return rate: 53%). The results of RQ1 shown in Table 1 include data on head nurse leadership style, staff nurse demographics, and staff nurse clinical competency. The number of female participants was higher than that of male participants, the average age was 31.6 years, and more participants were single. A majority were educated to the university (baccalaureate) level, held the title of nurse, and worked in the surgical department. Their average length of employment was 8.66 years. The average scores of head nurses were 2.69 for overall leadership skill, 2.89 for transformational leadership style, and 2.49 for transactional leadership style. The clinical competency components ranked from highest to lowest score were patient care (M = 3.35), professionalism (M = 3.28), communication skills (M = 3.18), management (M = 2.84), and knowledge (M = 2.73).
Table 1 - Head Nurse Leadership and Staff Nurse Demographics and Clinical Competency Variables (N = 200) Variable n % Median IQR Gender a Male 11 5.5 Female 187 93.5 Age (years; M and SD) a 31.60 8.04 28.33 12.84 ≤ 30 115 57.5 31–40 49 24.6 41–50 31 15.6 > 50 4 2.0 Marital status a Single 146 73.0 Married 53 26.5 Level of education Junior college or below 9 4.5 University/college 178 89.0 Graduate school 13 6.5 Job title a Assistant head nurse 5 2.5 Nurse Leader 18 9.0 Staff nurse 174 87.0 Employment department Medicine 85 42.5 Surgery 90 45.0 Obstetrics & Gynecology 12 6.0 Pediatrics 10 5.0 Multiple departments 3 1.5 Length of employment (years; M and SD) 8.66 7.92 5.58 11.14 < 3 79 39.5 3–10 60 30.0 > 10 61 30.5 Mean SD Median IQR Head nurse overall leadership styles 2.69 0.66 2.78 0.95 Transformational leadership 2.89 0.87 3.00 1.47 Transactional leadership 2.49 0.59 2.50 0.80 Staff nurse clinical competency 3.08 0.49 3.09 0.65 Patient care 3.35 0.53 3.33 0.80 Professionalism 3.28 0.47 3.27 0.73 Knowledge 2.73 0.68 2.77 0.80 Communication 3.18 0.55 3.07 0.87 Management 2.84 0.65 2.87 0.80The results for RQ2, shown in Table 2, reveal significant differences in staff nurse clinical competency associated with age, marital status, level of education, job title, and length of employment. Age was associated with clinical competency (χ2 = 23.55, p < .001) particularly in the domains of patient care (χ2 = 22.18, p < .001), professionalism (χ2 = 13.17, p < .05), knowledge (χ2 = 32.99, p < .001), communication skills (χ2 = 19.61, p < .001), and management (χ2 = 24.86, p < .001). Staff nurses aged 41–50 years earned better scores than those younger than 30 years old in terms of overall competency, patient care, professionalism, knowledge, and communication. Staff nurses over 50 years old were more competent in communication and management than those younger than 30 years old. Staff nurses aged 31–40 years demonstrated a higher level of competency in knowledge than those younger than 30 years old. Staff nurses aged 41–50 years demonstrated a higher level of competency in knowledge than those aged 31–40 years. Married nurses scored higher in overall competency, patient care, professionalism, knowledge, communication, and management than single nurses. The marital status of staff nurses was associated with clinical competency (Z = −3.46, p < .001), particularly in terms of patient care (Z = −3.95, p < .001), professionalism (Z = −2.29, p < .05), knowledge (Z = −4.04, p < .001), communication skills (Z = −2.22, p < .05), and management (Z = −3.06, p < .05). The educational level of staff nurses was associated with clinical competency (χ2 = 9.82, p < .05), particularly in terms of patient care (χ2 = 8.73, p < .05), professionalism (χ2 = 7.88, p < .05), knowledge (χ2 = 14.46, p < .001), communication skills (χ2 = 6.51, p < .05), and management (χ2 = 8.54, p < .05). Post hoc comparisons revealed no significant effect of educational level on communication skills. Compared with nurses educated to the junior college level or below, nurses with a master's degree showed higher levels of competency in the following domains: overall competency, patient care, professionalism, knowledge, and management. Compared with nurses educated to the college or university level, nurses holding a master's degree showed higher levels of competency in the following: overall competency, patient care, knowledge, and management. The job title “staff nurse” was found to influence clinical competency (χ2 = 16.69, p < .001), particularly in terms of patient care (χ2 = 8.78, p < .05), professionalism (χ2 = 11.30, p < .05), knowledge (χ2 = 27.57, p < .001), communication skills (χ2 = 15.43, p < .001), and management (χ2 = 18.36, p < .001). Nurse leaders were more competent in overall competency, patient care, professionalism, knowledge, communication skills, and management than staff nurses. Assistant head nurses showed greater knowledge than staff nurses. Also, employment length was found to influence clinical competency (χ2 = 22.03, p < .001), particularly in terms of patient care (χ2 = 33.82, p < .001), professionalism (χ2 = 6.92, p < .05), knowledge (χ2 = 27.13, p < .001), communication skills (χ2 = 19.40, p < .001), and management (χ2 = 18.58, p < .001). Those with employment lengths of 3–10 years demonstrated higher levels of overall competency, patient care, knowledge, communication, and management competency than their peers with less than 3 years of employment experience. Also, those with employment lengths > 10 years demonstrated greater overall competency, patient care, knowledge, communication, and management competency than nurses employed for less than 3 years. Post hoc comparisons revealed no significant effect of employment length on professionalism.
Table 2 - The Effects of Demographic Variables on Clinical Competency (N = 200) Variable χ2/Z Value Overall Clinical Competency Patient Care Professionalism Knowledge Communication Skills Management Gender −0.37 −0.58 −0.73 −1.06 −0.57 −0.53 Male Female Age (years) 23.55** 22.18** 13.17* 32.99** 19.61** 24.86** ① ≤ 30 ③>① ③>① ③>① ③>①,
Comments (0)