
Remember me



Rectal cancer is a common type of tumor with a high incidence and mortality rate worldwide (Sung et al., 2021). Surgery is the primary treatment for rectal cancers, and low anterior resection is widely used in anal-sparing surgeries (Du et al., 2021). Temporary fecal diversion has been utilized alongside anterior resections for decades to protect the anus as much as possible and prevent anastomotic fistulas, which are the most severe postoperative complication (Gu & Wu, 2015). Loop transverse colostomy and loop ileostomy (LI) are common types of temporary diverting stomas.
Evidence-based studies have shown that LI has fewer complications during ostomy formation and reversal than loop transverse colostomy (Du et al., 2021; Gavriilidis et al., 2019; Güenaga et al., 2007). Therefore, LI is the leading temporary fecal diversion procedure. However, the high stool output after ileostomy and the large number of digestive enzymes in the anal discharge increase the challenge of proper ileostomy care. Improper care practices, for example, frequently changing appliances and consuming high-sugar foods, significantly increase the risk of complications such as peristomal dermatitis and dehydration (Chudner et al., 2019; Du et al., 2021). The primary focus of colorectal surgical care is the professional direction and supervision of patients with ileostomies through, for example, the provision of standardized dietary recommendations and discharge care programs by enterostomal therapists.
The enhanced recovery after surgery (ERAS) program is an evidence-based and multidisciplinary perioperative care pathway that has been shown to reduce postoperative complication rates, hospitalization duration, and costs and is becoming the standard of care and best practice in many surgical specialties around the world (Ljungqvist et al., 2017, 2021). The ERAS program imposes new requirements in several areas of perioperative care, including bowel preparation, rehabilitation training, and nutritional correction (Carli et al., 2020; Ripollés-Melchor, Abad-Motos, Cecconi, et al., 2022). These changes, especially related to the substantially reduced hospitalization durations, disrupt standard care plans and generate new patient care demands. In addition, most existing ERAS programs are based on expert consensus and lack consideration of the patient perspective, undermining patient compliance rates and intervention effects (Fischer et al., 2021; Forsmo et al., 2016). The care requirements of patients under the new ERAS paradigm have yet to be extensively studied.
Supportive care aims to provide cancer patients with the services necessary to meet their informational, emotional, social, and physical needs throughout the cancer treatment trajectory (Kotronoulas et al., 2017). Identifying supportive care needs (SCNs) is fundamental to designing effective cancer care programs. Caring for patients with rectal cancer with temporary ostomy is one of the most challenging and complex aspects of clinical cancer care, as these patients have substantial SCNs. Furthermore, the application of ERAS in the surgical treatment of colorectal cancer presents additional challenges and SCNs for patients. The SCNs of patients with colorectal cancer were investigated in this study using a mixed approach to provide a reference for the future development of related ERAS nursing care plans.
Methods Study DesignA convergent parallel mixed-methods design was used to collect quantitative and qualitative data concurrently. The quantitative component of this study involved conducting a cross-sectional questionnaire-based survey to determine the content and level of SCNs in patients with rectal cancer with temporary ostomy in the ERAS protocol. The qualitative component involved conducting semistructured individual interviews with individual patients to further elucidate the content of SCNs.
Setting and ParticipantsIn the quantitative component of this study, patients with rectal cancer with temporary ostomy were recruited using a convenience sampling method between March and June 2020 at the gastrointestinal surgery ward and wound & ostomy clinic of two public tertiary hospitals in Changchun, Jilin Province, China. Eligibility criteria were patients who (a) were 18 years or older, (b) were diagnosed with primary rectal cancer, (c) had received radical rectal cancer surgery and temporary ostomy under the ERAS protocol for the first time, and (d) voluntarily provided informed consent to participate. Exclusion criteria were (a) being unaware of their illness, (b) having a temporary ostomy for other reasons (trauma, ulcerative colitis, etc.), and (c) having a psychiatric disorder or hearing impairment.
In the qualitative component of this study, 13 of the participants from the quantitative component were selected using maximum variation sampling for participation in semistructured interviews. A maximum variation sample was constructed by identifying the critical dimensions of variations and then selecting those participants who differ as much as possible from each other in terms of these dimensions (Benoot et al., 2016). The dimensions considered included (a) background (age, gender, educational level, and place of residence) and (b) duration of living with a temporary stoma (perioperative period, 1–6 months after the operation and more than 6 months, the latter of which is classified as delayed closure of temporary ostomy).
Data CollectionIn the quantitative component of this study, the participants completed the questionnaire, which collected data in three categories: demographics (age, gender, and educational level), clinical characteristics (type of stoma, duration with stoma), and SCNs. The general characteristics data, including the demographics information and duration with stoma, were obtained from self-reports and medical records. The Supportive Care Needs Survey Short Form 34 was used to assess the unmet SCNs of participants in five domains: physical and daily living needs (five items), psychological needs (10 items), health system and informational needs (11 items), care and support needs (five items), and sexual needs (three items; Boyes et al., 2009). The participants were asked to rate the need intensity of each over the past month on a 5-point Likert scale: 1 = no need: not applicable, 2 = no need: satisfied, 3 = low need, 4 = moderate need, and 5 = high need. The Chinese version of the SCN survey form has been previously validated for good reliability and validity (Au et al., 2011) and has been widely used to assess the needs of patients with breast and colorectal cancers (Lam et al., 2016; Li et al., 2013).
Preliminary interview guidelines for the qualitative component of this study were prepared based on prior research and the advice of medical experts (one senior doctor and one nurse). The guideline was modified based on the results of a preinterview conducted on two patients with temporary ostomies. The content and sequence of questions included introductory, central, and closing questions following the structure developed by Krueger and Casey (2014). The following questions were asked to obtain qualitative data: “What did you experience after receiving a temporary ostomy under the ERAS protocol?”, “What did you find most difficult during this period?”, “What kind of help/support did you receive during this time?”, and “What kind of help/support did you need most during this time?”
Ethical ConsiderationsThis study was reviewed and granted exempt status by the ethics committee of the First Hospital of Jilin University (No. 2020-454). The study purpose and methods were clearly explained to the participants, whose anonymity and confidentiality were maintained.
Study RigorStudy rigor was enhanced by triangulating among data sources (Carter et al., 2014), data collection methods, and researchers. Recruiting participants from different hospitals (two tertiary public hospitals) and settings (wards and wound & ostomy clinic) triangulates data sources and helps maximize diversity among study subjects; using different data collection methods, including interviews, observations, and field notes, facilitates triangulation and increases study credibility; and using two researchers to conduct surveys, interviews, and data analysis promotes diversity in observations and findings.
Data AnalysisQuantitative data were analyzed in this study using IBM SPSS Statistics 23.0 (IBM Inc., Armonk, NY, USA). Demographic, clinical characteristic, and SCN data were analyzed using frequency and percentage (count data) and mean and standard deviation (measurement data). In the qualitative component, the semistructured individual interviews were conducted for 30–50 minutes each. Within 24 hours of each interview, the audio was transcribed word for word, and the textual data were supplemented using verbal and nonverbal behavioral records for each participant noted during the interview. All data were analyzed separately by two researchers using the thematic analysis method.
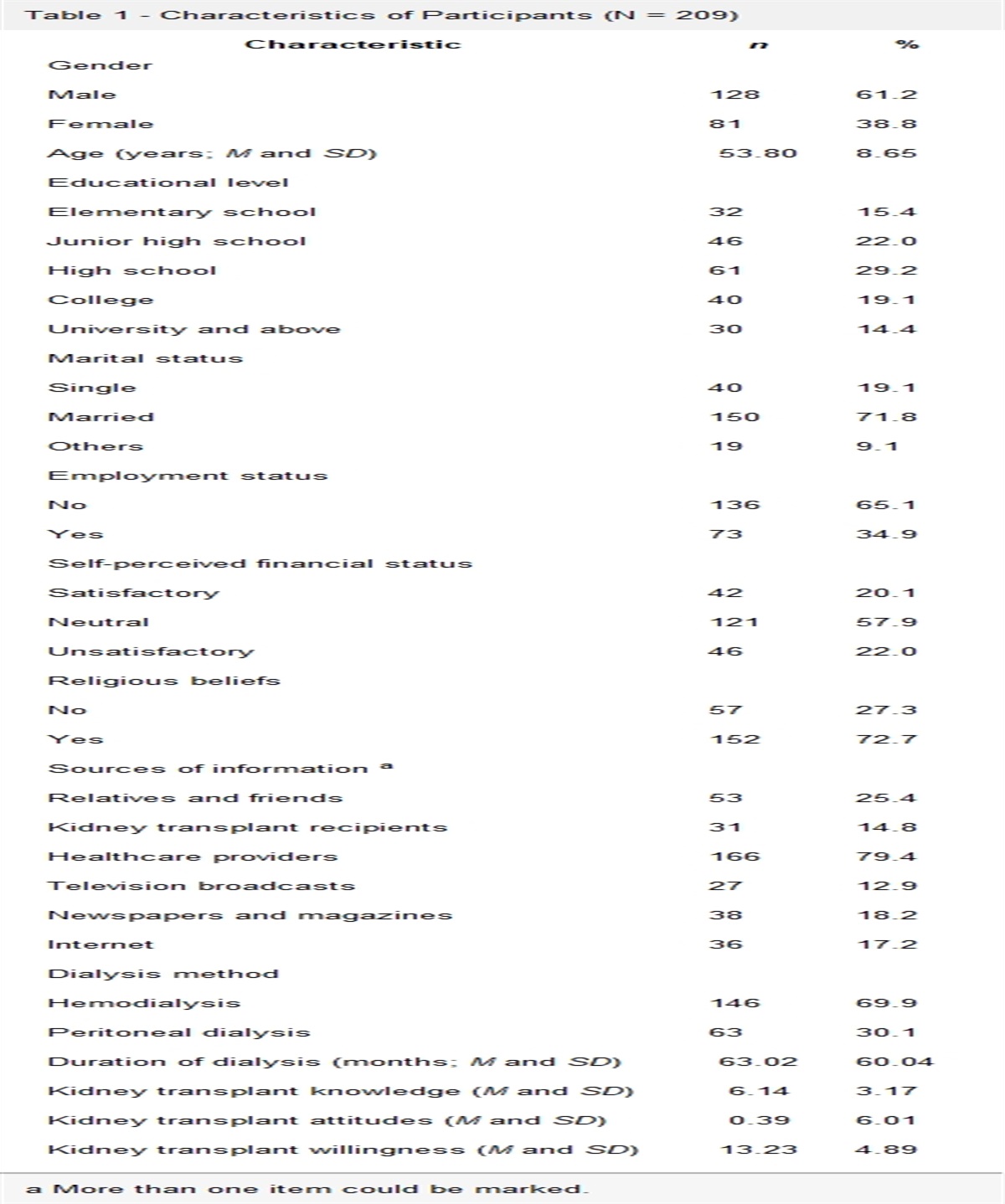
Results Quantitative ResultsAmong the 140 participants in the quantitative component of this study, 57.9% were male, most (76.4%) were over 50 years old, 45.7% suffered from one or more chronic diseases, and 67.9% had lived with ostomy for 1–3 months (Table 1).
Table 1 - General Characteristics of Participants in the Quantitative Component (N = 140) Variable n % Gender Male 81 57.9 Female 59 42.1 Age (years) ≤ 40 11 7.9 41–50 22 15.7 51–60 50 35.7 61–70 40 28.6 ≥ 71 17 12.1 Educational level Primary school 21 15.0 Junior high school 51 36.4 High school 25 17.9 College degree 21 15.0 Bachelor's degree or above 22 15.7 Marital status Married 118 84.3 Divorced 1 0.7 Widowed 19 13.6 Unmarried 2 1.4 Occupational status Retirement 52 37.1 Employed 31 22.1 Unemployment 31 22.1 Other 26 18.6 Residence City 92 65.7 Rural 48 34.3 Residence style Solitary 15 10.7 Living with family 125 89.3 Living in a nursing facility 0 0.0 Other 0 0.0 Chronic diseases None 76 54.3 One 33 23.6 Two 22 15.7 Three or more 9 6.4 Medical payment method Self-financed 18 12.9 Employee health insurance 55 39.3 Resident health insurance 20 14.3 Medical insurance for retired executives 8 5.7 New rural cooperative medical system 39 27.9 Monthly per capita household income Business insurance 0 0.0 < 1,000 33 23.6 1,000–3,000 57 40.7 3,001–5,000 32 22.9 > 5,000 18 12.9 Primary caregiver Spouse 90 64.3 Children 47 33.6 Siblings 3 2.1 Others 0 0.0 Type of stoma Ileostomy 138 98.6 Colostomy 2 1.4 Duration with stoma (months) 1–3 95 67.9 4–6 12 8.6 7–12 14 10.0 > 12 19 13.6“Health system and informational needs” earned the highest average score of 61.72, followed by “care and support needs” (49.43). Sexual needs earned the lowest average score of 20 (Table 2). The analysis of individual items found that the 10 items with the highest scores were all in the domain of health system and informational needs, with unmet need rates between 70.0% and 81.4%. The three items with the lowest scores were all in the domain of sexual needs, with unmet need rates between 22.1% and 27.1% (Table 3).
Table 2 - Scores for Each Domain of Supportive Care Needs (N = 140) Domain Minimum Maximum M SD Physical and daily living needs 0.00 90.00 38.93 22.22 Psychological needs 0.00 100.00 46.34 26.91 Sexual needs 0.00 100.00 20.00 23.88 Care and support needs 0.00 100.00 49.43 31.90 Health system and information needs 0.00 100.00 61.72 30.38Note. H = health system and information needs; P = psychological needs; D = physical and daily living needs; C = care and support needs; S = sexual needs.
Thirteen patients participated in the qualitative component of this study, including six men and seven women aged 38–80 years. These patients had lived with ostomy for periods between 5 days and 13 months (Table 4). Five main themes emerged after analysis of the transcripts, with the descriptions of the themes and subthemes shown in Table 5.
Table 4 - General Characteristics of Respondents in the Qualitative Component (N = 13) No. Gender Age (Years) Educational Level Residence Type of Stoma Time Living With Stoma OP1 Male 68 Junior high school City Ileostomy 5 days OP2 Male 38 Bachelor's degree City Ileostomy 2 months OP3 Male 43 Junior high school Rural Ileostomy 3 months OP4 Female 70 Primary school City Ileostomy 5 months OP5 Female 53 Primary school Rural Ileostomy 5 days OP6 Male 62 Junior high school City Ileostomy 6 months OP7 Female 57 High school City Ileostomy 10 months OP8 Female 77 Primary school City Ileostomy 8 months OP9 Female 51 High school City Ileostomy 5 months OP10 Male 63 College degree City Ileostomy 3 months OP11 Male 80 Primary school Rural Colostomy 12 months OP12 Female 69 Junior high school City Ileostomy 13 months OP13 Female 61 High school City Ileostomy 1 months
Comments (0)