
Remember me



Person-centered care (PCC) is an approach to healthcare that focuses on the individual needs, preferences, and values of patients (American Geriatrics Society Expert Panel on Person-Centered Care, 2016). Moreover, PCC involves viewing patients as whole persons and encourages patients to be treated with empathy, respect, and dignity and be involved in decisions about their care (Charalambous et al., 2012; Lusk & Fater, 2013). PCC is particularly important in the context of caring for older adults in nursing homes (NHs) who require physical, functional, and behavioral assistance in daily living due to dementia. Numerous PCC interventions involving social contact, physical activities, cognitive training, sensory enhancement, assistance with daily living, and environmental adjustments have been developed for residents with dementia in NH settings (Mohr et al., 2021). These interventions have resulted in positive outcomes for both residents (e.g., improved quality of care, quality of life, and satisfaction) and NH nursing staff (e.g., increased job satisfaction, retention, and work empowerment; Brownie & Nancarrow, 2013; Edvardsson et al., 2011; Silén et al., 2019).
In addition, PCC has been shown to be effective in managing the behavioral and psychological symptoms of dementia (BPSD), which refer to the range of noncognitive symptoms such as agitation, aggression, and wandering commonly seen in NH residents (Kales et al., 2015, 2019; Kolanowski et al., 2017; Li & Porock, 2014). The PCC approach, which helps ensure care is tailored to the unique needs and preferences of each resident, recognizes that the behavior of residents with BPSD is often a response to unmet needs or unaddressed physical or psychological discomfort (J. Y. Lee et al., 2023). Understanding and identifying the underlying problems of individual residents are important components of the BPSD care competence of NH nurses, who play pivotal roles in providing direct care to residents with BPSD (D. Kim et al., 2022). The aim of PCC interventions for BPSD such as reminiscence, music, cognitive, and multisensory stimulative therapies (K. H. Lee et al., 2022) is to provide a safe and supportive environment that promotes independence, social engagement, and meaningful activities while minimizing the use of restrictive interventions and medications (Kales et al., 2015; Sefcik et al., 2020), resulting in a reduction in antipsychotics use and the incidence of BPSD (Fossey et al., 2014; K. H. Lee et al., 2022).
However, due to the complex nature of PCC, implementation strategies vary widely among NHs and individual staffs (Dys et al., 2022; Güney et al., 2021) due to factors associated with individual nurses, differences in NH environments, and differences in national/regional norms (E. L. Brown et al., 2020). These differences contribute to significant heterogeneity in the PCC approaches employed at NHs (Mohr et al., 2021). Moreover, some studies have found that, although nurses may express support for PCC in principle, systemic and practical obstacles often prevent them from fully implementing PCC in NH practice (Güney et al., 2021; J. Y. Lee et al., 2023). Additionally, nurses often face conflicts between resident preferences and medically indicated situations or safety concerns (Kusmaul & Tucker, 2020; Parker et al., 2019) as well as common problematic issues caused by residents with BPSD (Kales et al., 2015). Despite its importance, PCC is difficult to effectively implement in managing BPSD in NHs (Oppert et al., 2018; Sefcik et al., 2020).
Understanding how nurses perceive and approach PCC in the context of BPSD management can help identify barriers to and facilitators of PCC implementation in this context. Nurses are the frontline care providers in NHs, and their perceptions and attitudes towards PCC can significantly impact the quality of care received by residents (Dys et al., 2022). Gaining insight into nurses' subjective perspectives on providing PCC in managing BPSD in NHs may elicit a deeper understanding of how nurses interpret and approach the provision of PCC as well as of the various factors that influence their ability and willingness to provide PCC in this context (Watts & Stenner, 2012). Therefore, in this article, Q methodology is used to explore the subjectivity in PCC in managing BPSD of residents of NHs.
MethodsQ methodology, developed by William Stephenson, is a research technique that combines qualitative and quantitative methods to study subjective viewpoints (S. R. Brown, 1980; Watts & Stenner, 2012), using a structured procedure to explore the different subjective perspectives and experiences of participants regarding complex issues (Stephenson, 1953; Watts & Stenner, 2012). The five steps to conducting Q methodology include (a) developing a Q-population, (b) selecting a Q-sample, (c) selecting a P-sample, (d) conducting Q-sorting, and (e) analyzing and interpreting the Q-sorts.
Q-Population Development and Q-Sample SelectionA Q-population (aka “concourse”) is a list of statements that encompass a broad range of a research topic (Stephenson, 1953; Watts & Stenner, 2012). The Q-population may be acquired from the literature, interviews, newspapers, and other suitable sources (S. R. Brown, 1980). In this study, the Q-population was acquired using semistructured interviews during which self-referent statements related to providing PCC in managing BPSD were collected.
Ten nurses with more than 3 years of experience providing BPSD care in NHs were purposively recruited for the interviews (Benner, 1982). All of the participants were female; three held a master's degree or higher, and the others held bachelor's degrees; their average age was 52.2 (SD = 8.09) years; and their average years of experience in BPSD care was 6.6 (SD = 3.27) years. The interviews were conducted during January and February 2022 via telephone or Zoom because of COVID-19 infection concerns. The interview questions were developed using a review of the literature on PCC in NHs. The participants were asked to provide self-referential statements by answering questions such as “How do you judge what references to use to provide care for residents with BPSD while considering their values, characteristics, and preferences?” and “What is important for providing PCC in managing BPSD, and why?”
From the interview transcriptions, 71 statements related to PCC in managing BPSD in NHs were collected. After eliminating ambiguity and duplication, a final set of 43 clear and distinct statements were selected as the Q-sample (Table 1). Finally, two nursing professors with experience in Q methodology reviewed the Q-sample for readability and distinctiveness in representing PCC in managing BPSD in NHs.
Table 1 - Statements and Factor Arrays of the Q-Sample Q-Sample Factor Arrays I II III IV 1. a I believe that how the resident's BPSD was managed before admission to NHs is irrelevant to setting the direction of care in a person-centered way. −4 −3 −2 −3 2. I ask the resident's family if there were any special events in the resident's life to find out the underlying causes of the resident's BPSD. 2 0 1 3 3. Even when a resident is talking to a care worker, I listen to the resident's words and actions to gather clues about the cause of BPSD. 3 1 2 2 4. If a resident continues to shout despite any method I use, I think of a new method that was effective in different situations in the past and try it on the resident. 4 3 0* 2 5. If a resident is single or does not have family, it is difficult for me to determine how to effectively approach them personally when their BPSD appears. 1* 3** 0 −1 6. a I think it's not the best way to relieve BPSD symptoms by identifying different individual characteristics for each resident and providing person-centered care based on them. −3 2** −2* −4 7. Even if the conversation with the resident has accumulated for a long time, it is difficult to know what the best individualized approach is when their BPSD appears. 0 −1 1 1 8. a Close observation and conversation with the resident are not necessary for setting individual standards for how far the resident can think and act on their own. −1 0* −3 −2 9. To truly understand the resident well, it is necessary to give them time to fully adapt to the NH and express themselves comfortably. 1** 4 4 4 10. The resident's daily condition determines how their day will pass, so I first identify the condition and atmosphere of individual residents every day. −1** 4 3 4 11. a Providing personalized care has nothing to do with respecting the dignity of the resident. −4 −4 −3 −2 12. a Residents cannot be directly involved in determining the direction of individualized care throughout nursing planning and intervention. −4 −4 −1** −4 13. a In a situation where the resident refuse to do so, I make it a more important criterion to keep the direction of the nursing plan than to respect the autonomy of the resident. −3 0 −2 0 14. Based on what I aware about the resident, I set a safe standard for the individual resident to accept BPSD without any intervention. 2** −1 0 −1 15. I think NHs are a place where person-centered care can be effectively provided by focusing on personality and characteristics rather than labeling the resident by diagnosis or symptom name. 3 2 −1 −1 16. a Rather than the words and actions of the residents, it is necessary to restrict them to act as I see and judge on them. −2 −1 −1 0 17. a I believe that making an effort to establish a close relationship with resident results in understanding their personal values and preferences. −2 2** −3 −3 18. To give the feeling that I know the residents well, I try to investigate past life events or information about residents in advance and understand their words and actions based on them. 1 1 0 4** 19. a It is impossible to maintain a true trust relationship with individual residents because they have poor cognitive function due to dementia. −2 −3 −4 0** 20. a Even if I am usually kind to the residents, they may not feel that I truly understand their personal emotional needs. 0 −4 −3 −1 21. To identify and solve the underlying emotional needs of individual residents, I observe and act the same way the residents behave. 0 −3 0 −2 22. a Focusing on the cause of BPSD rather than understanding what is important to the residents and recognizing their needs in advance is less important in providing person-centered care. 0 −2** 1 0 23. Being a person who can better understand and explain the needs of the residents than their family is the most important thing in personalized BPSD care. 0 0 1 0 24. I treat the residents kindly and open-mindedly with the aim of becoming a person who can personally talk and express what they need at any time. 2 1 3* 2 25. I am always careful about my behavior and attitude and maintain the same mood and appearance every time because the words or actions I inadvertently say can be interpreted differently by individual residents and may lead to BPSD. −1** 3 4 3 26. I believe that BPSD can be alleviated if residents feel a sense of belonging to our facility, so I actively think of ways to foster positive relationships among residents. 0* 3 2 2 27. With the goal of establishing a sense of personal trust with residents, I listen carefully to whatever they have to say. 3 1* 2 −1* 28. The interaction between residents with BPSD and myself is a delicate relationship that requires sensitivity to even small changes, so I am mindful of my words and actions to maintain consistency. 1 1 3* 1 29. a It's irrelevant to planning and effectively implementing personalized care to inform the residents or their family members of the current BPSD status and the direction of care. −3 2** −1* −4 30. a I don't think sitting next to the residents without any special conversation or activity affects my relationship with the individual residents. −1 −1 −2 1** 31. a To provide proper person-centered care, I think it is important to be good to the residents rather than to cooperate with other staff. −3 −3 −4 −2 32. To provide personalized care, I actively accept opinions and suggestions from residents and family members and use them to establish care strategies. 4 2 1 2 33. To improve BPSD in residents, I should promptly share any new characteristics or effective care methods with other staff. 2 −2** 2 3* 34. a While other staff members may have a different perspective, I don't think that understanding residents and their BPSD requires considering all viewpoints. 0 −2 −4 −2 35. a Person-centered care is only possible for the resident with mild dementia or without dementia, but it is practically difficult for the resident with BPSD. −2 1** −1 −3 36. Observing residents' conditions and regularly consulting with other staff is important for updating nursing strategies and providing effective person-centered care. 3* 0 0 1 37. Not only me but also other staff and the resident's relationship should be kept consistent, so I share the condition and the levels of function of individual residents with other staff. 4** −1 2** −1 38. a Because I have a good trust relationship with the residents, maintaining residents' good social relationships with other residents and staff members is not important. −2* −1 0 0 39. a I don't think there is a need to involve the family in the process of person-centered care because the participation of the family does not help the residents relieve BPSD. −1 −2 −1 −3 40. Ultimately, I think that providing person-centered care is about ensuring autonomy for residents in NHs. 1* 4 3 3 41. If the residents describe the NH as “my home” and feel comfortable, I consider it a successful personalized approach. 1 −2** 4** 1 42. Cooperation with other staff and the director is necessary to create a comfortable environment tailored to individual residents in the NH. 2 0 1 0 43. a I don't think the personalized approach in managing BPSD is related to the resident feeling our NH is safe and stable. −1 0 −2 1Note. BPSD = behavioral and psychological symptoms of dementia; NH = nursing home.
a Reversed statements.
*p < .05. **p < .01.
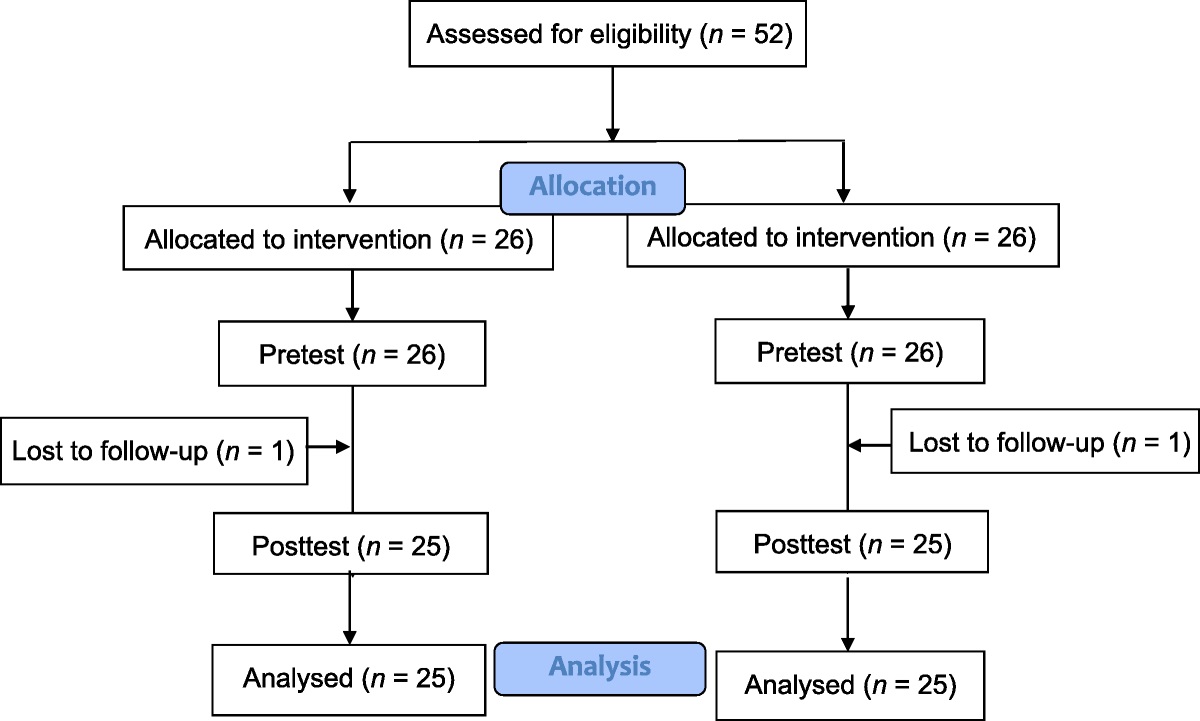
In line with Q methodology, the participants were asked to sort a set of statements or items based on their subjective perspective (Watts & Stenner, 2012) in a process known as “Q-sorting.” The participants who performed the sorting were the “P-sample” (S. R. Brown, 1980; Stephenson, 1953), which is a variable of analysis in Q methodology for which a small size is sufficient to make clear distinctions among intraindividual differences (S. R. Brown, 1980; Watts & Stenner, 2012). Half of the number of the Q-sample in this study (i.e., 21) was the recommended minimum size of the P-sample (Stone & Turale, 2015; Watts & Stenner, 2012). In this study, participants were recruited through NH directors, who served as gatekeepers. An informative letter was distributed to explain the research purpose and procedures. To ensure sample variance, five NHs with resident capacities ranging from 49 to 320 were selected. For the P-sample, 30 NH nurses with more than 3 years of experience in providing direct care to residents with BPSD were purposively recruited.
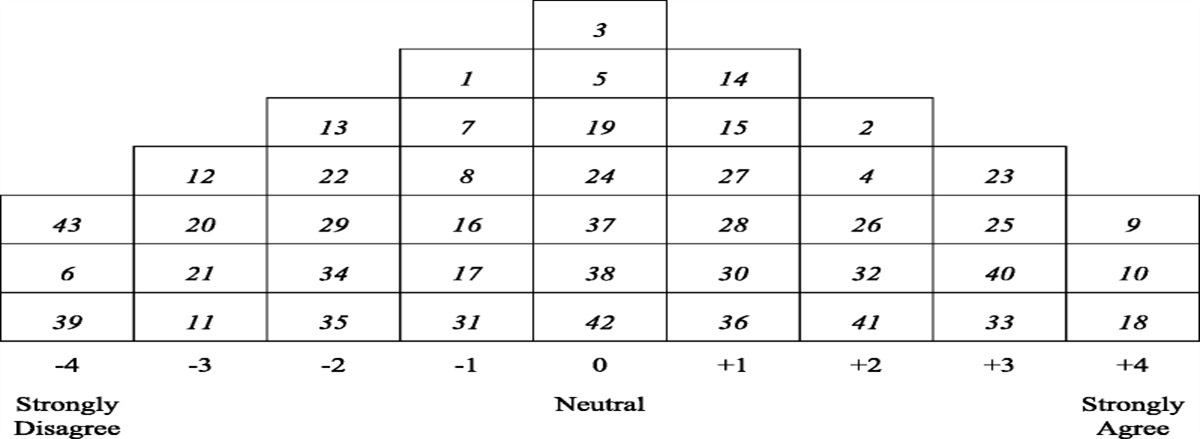
Q-SortingQ-sorting includes a card sorting activity and postsorting interviews. In this step, the participants (P-sample) classified cards into three clusters of “disagree,” “neutral,” and “agree” with regard to the statement written on each card. Questions were given to the participants to facilitate sorting, such as “Place cards that you disagree with on the left, agree with on the right, and put neutral statements in the middle.” The participants then placed the cards on a preestablished Q-sort grid in the form of a quasi-normal distribution by putting the ones they most disagreed with on the −4 section and most agreed with on the +4 section (Figure 1). After sorting was completed, a postsorting interview was conducted with the P-sample to ask about the reasoning behind their chosen distributions, with an emphasis on the cards placed at the extremes of the grid.
 Figure 1:
Figure 1: Example of a Completed Q-Sorting Grid (Participant 1)
Table 2 - Eigenvalues and Total Variances, by Factor Component Factor IAmong the 30 NH nurses recruited for the P-sample, one was excluded due to having contracted COVID-19. Consequently, 29 sorts were included in the analysis. The Q-sorting activity was conducted from May to June 2022 using Zoom due to COVID-19 concerns. The sorting process was video and audio recorded, and the researchers composed and shared field notes on their observations of the participants' responses.
Data Analysis and Interpretationn Q methodology, an inverted factor analysis is used in which data are analyzed to identify the associations among participants (i.e., by person) rather than among specific traits or statements (i.e., by variable; Watts & Stenner, 2012). The aim of Q-factor analysis is to identify patterns in sorting across participants to identify patterns and clusters of similar viewpoints, which are referred to as factors and which represent shared perspectives on a particular topic (S. R. Brown, 1980; Watts & Stenner, 2012). PQMethod 2.35, a statistical program designed for Q-factor analysis, was used to derive the factors in this study (Schmolck, 2021). Following centroid factor analysis and varimax rotation, four factors were determined using the criteria that each had earned eigenvalues higher than 1, maximized defining significant statements, and had more than two defining sorts (Watts & Stenner, 2012).
Whereas analysis is quantitative, factor interpretation is a qualitative process in the Q methodology. Factor arrays (Table 1); a crib sheet, which is a tool designed for assisting in the detailed interpretation of the identified factors by listing the cards located at the extremes of the grid; distinguishing statements; and consensus statements for each factor were utilized (Watts & Stenner, 2012). Moreover, the postinterview data and P-sample's demographic data were included in factor interpretation. Finally, the labeling of each factor was completed after a discussion was held regarding the representativeness of factors in distinguishing the viewpoints among NH nurses on PCC in managing BPSD.
Ethical ConsiderationsThis study was approved by the institutional review board of the university (KUIRB-2020-0234-02). All participants were given written consent forms that included comprehensive information about the research and guarantees of their confidentiality.
ResultTwenty-nine NH nurses participated in the Q-sorting procedure. Four factors were found to explain 76% of the total variance (Table 2). Also, 27 of the Q-sorts (93.1%) were significantly loaded on a single factor (p < .01), whereas two of the Q-sorts did not load significantly on any factor. The general characteristics of the participants and each factor are presented in Table 3. After reviewing the factor arrays, crib sheets, postinterview transcriptions, and demographic data, the following four subjective frames for PCC in managing BPSD by NHs nurses emerged: “sharing information focused on details to update care strategies,” “monitoring until the true needs of residents are identified,” “being aware of interactive cues in relationships,” and “connecting an individual's life pattern to their current care.”
Factor 1: Sharing Information Focused on Details to Update Care StrategiesFactor 1 accounted for 59% of the total variance and earned an eigenvalue of 16.99. Ten of the participants significantly loaded on this factor. The Q-sample that this factor significantly agreed with included Statements 37 (+4) and 36 (+3), indicating that sharing information about residents' conditions is a priority factor involved in PCC in the context of BPSD management. The participants prioritized closely assessing residents with BPSD and sharing new information with other staff to establish a standard for providing personalized care (Q-sample 14, hereafter referred to as Q-14) and maintaining trusting relationships with residents (Q-38).
Participant 18, whose sort had the highest load on this factor, spoke about how updating residents' information through collaborative conversations with other staff members is important for consistent and effective PCC:
It is necessary to understand the resident’s latest condition based on shared information rather than relying solely on my own thoughts and judgments to provide an appropriate personalized approach. Since it is not possible to be with residents 24 hours a day, it is essential to share various attempts and experiences concerning BPSD care strategies by identifying and communicating the symptoms and conditions of residents at different times, environments, and spaces.
However, the participants tended to perceive understanding the feelings (Q-22) and identifying the emotional needs (Q-20, Q-22) of residents as less important. Rather than focusing on providing emotional stability, the participants who loaded on this factor tended to focus on integrating the perspectives of other staff to make better decisions. Participants emphasized that PCC for BPSD in NHs should take an interprofessional approach because NHs are where residents will live for the rest of their lives with support from multiple healthcare professionals, including nurses, social workers, physical therapists, and nutritionists. Participant 28, who weighted second highest on this factor, said:
If I believe that I'm the only one responsible for providing good care to the resident. True personalized nursing cannot be achieved. I think that providing stable and consistent care, where all NH staff possess the right information and practice in the same direction, is essential for personalized BPSD nursing so that the resident doesn't become confused.
Factor 2: Monitoring Until the True Needs of Residents Are IdentifiedFactor 2 included four significant Q-sorts of NH nurses, accounting for 7% of the total variance and earning an eigenvalue of 2.13. On average, the participants who loaded on this factor were younger in age (mean age is 49.0 [SD = 9.8] years) and had less NH working experience (mean is 4.8 [SD = 1.7] years) than the overall P-sample (52.3 ± 8.4 and 6.3 ± 3.0
Comments (0)