
Remember me



Fatigue is a highly prevalent symptom among patients with end-stage renal disease who receive hemodialysis (Davey et al., 2019). Fatigue refers to a subjective and persistent sense of physical and/or emotional tiredness, weakness, exhaustion, and lack of energy that precludes daily activities or tasks and may interfere with normal functioning (Gregg et al., 2021; Menting et al., 2018). Fatigue following hemodialysis has been linked with impaired quality of life, cognitive impairments, negative emotions, and sleep disturbances (Davey et al., 2019; Jaime-Lara et al., 2020), encouraging scholars to step up efforts to find an effective treatment to relieve fatigue in patients receiving hemodialysis.
Pharmacological therapy (i.e., Vitamin C and L-carnitine) has been proposed to relieve fatigue in patients with end-stage renal disease undergoing hemodialysis (Borran et al., 2021; Nishioka et al., 2022). However, evidence regarding this and other pharmacological interventions have been inconclusive, leading patients to seek nonpharmacological alternatives such as exercise (Malini et al., 2022) to relieve posthemodialysis fatigue. Acupressure, a traditional Chinese therapy that involves stimulating the energy pathways (meridians) throughout the body to increase the flow of qi, may help alleviate the symptoms of fatigue (Y. Cho et al., 2021; Khalid et al., 2021; Mehta et al., 2016). Acupressure is a manual technique applied using pressure from a finger, hand, elbow, or seed that stimulates specific acupoints on the body surface (e.g., limbs, trunk, ear, scalp, and wrist; Li et al., 2015). As a low-cost, easy-to-perform, noninvasive, and minimally risky treatment option, acupressure may be integrated into nursing practice (Lindquist et al., 2018) as well as daily care performed by patients and their caregivers.
The effects of acupressure on fatigue have been demonstrated in different populations. A recent meta-analysis (Hsieh et al., 2021) that included 14 randomized controlled trials (RCTs) with 776 patients with cancer demonstrated that the patients in the acupressure groups had lower average cancer-related fatigue than those in the control groups. Another meta-analysis study (Yang et al., 2015) that included two RCTs revealed acupressure as effective in reducing fatigue in patients receiving hemodialysis. However, more trials have been published since these previous meta-analyses, and the discrete effects of acupressure on the several domains of fatigue (e.g., mental fatigue) after hemodialysis have yet to be investigated. Furthermore, prior meta-analyses did not identify effective acupoints for fatigue reduction among patients receiving hemodialysis. If the effects of acupressure on posthemodialysis fatigue are supported, healthcare providers, patients, and caregivers may be trained to perform acupressure regularly to reduce posthemodialysis fatigue and improve patients' quality of life.
The purpose of this study was to comprehensively explore the effects of acupressure on fatigue in patients receiving hemodialysis. The moderating influences of bio-sociodemographic characteristics and methodology on the association between acupressure and posthemodialysis fatigue were also examined.
Methods Data Sources and SearchesThis meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (Page et al., 2021). The protocol for this review was registered at the International Prospective Register of Systematic Reviews on July 15, 2019 (registration number: CRD42019126268). To identify relevant studies, electronic databases including PubMed, Cochrane Central Register of Controlled Trials, and Embase were searched systematically for articles published up to November 2, 2022. To avoid publication bias, an additional search in ProQuest was conducted for relevant theses and dissertations during the same search period. Keyword combinations used to search for the studies were (Acupressure) AND (Fatigue) AND (hemodialysis OR ESRD OR “end stage renal disease” OR ESKD OR “end stage kidney disease” OR CKD OR “chronic kidney disease”). The reference lists of identified studies were also searched to include additional RCTs that may meet the eligibility criteria. No restriction on language or publication period was set.
Study SelectionEligibility criteria for participants (P), intervention (I), comparison (C), outcome (O), and study design (S) are detailed below:
Participants: Studies targeting patients aged 18 years and above who had been receiving hemodialysis for at least 3 months. Intervention: Studies in which acupressure (i.e., manual acupressure and auricular acupressure) was used as intervention arms. Comparison: Studies using a control group that received either usual care or acupoint stimulation (i.e., sham acupressure and transcutaneous electrical acupoint stimulation). Outcome: Studies reporting fatigue as a primary or secondary outcome. Study design: Prospective RCTs in which acupressure was used for fatigue relief that were also available as full publications in a peer-reviewed journal.The titles and abstracts were reviewed independently by two researchers to identify eligible articles from the search results. After deleting duplicates, the full-text articles were reviewed, and their data were analyzed.
Data Extraction and Risk-of-Bias AssessmentTwo of the researchers separately extracted data, including author name, year of publication, country, mean participant age, percentage of female participants, sample size, acupoints targeted, frequency of treatment, and assessment tools used, from all the included studies. Any disagreement in the extracted data was resolved through discussion with a third researcher until consensus was achieved.
To evaluate the internal validity of the included studies, two researchers assessed the methodological quality independently using the Cochrane Collaboration Risk of Bias 2.0 tool (Sterne et al., 2019). The five domains of bias evaluated included bias arising from the randomization process, bias due to deviations from the intended interventions, missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. The overall risk of bias was rated as one of three levels: “low risk of bias,” “high risk of bias,” or “some concern.” A third researcher was consulted to resolve discrepancies, with consensus reached through discussion.
Data Synthesis and AnalysisThe treatment effects of the study were estimated using Hedges's g, with corresponding confidence intervals derived from the differences in fatigue measurements between the pretreatment and posttreatment mean and standard deviations, and sample size. A random-effects model was used to estimate the treatment effects. Between-study heterogeneity was evaluated using Cochran Q and I2 statistics. The p value of the Q statistics was < .1, indicating substantial heterogeneity (Higgins et al., 2003), whereas the value of the I2 statistics ranged from 0 to 100, with higher scores indicating a higher degree of heterogeneity among the included studies. Furthermore, moderator and meta-regression analyses were conducted to detect potential moderators of the effects of acupressure on changes in fatigue in the presence of substantial heterogeneity. Also, Egger's intercept test (Egger et al., 1997) was used to test publication bias, with a significance level of < .05 indicating substantial publication bias. All the analyses in this study were performed on Comprehensive Meta-Analysis software, Version 2.0 (Biostat, Englewood, NJ, USA).
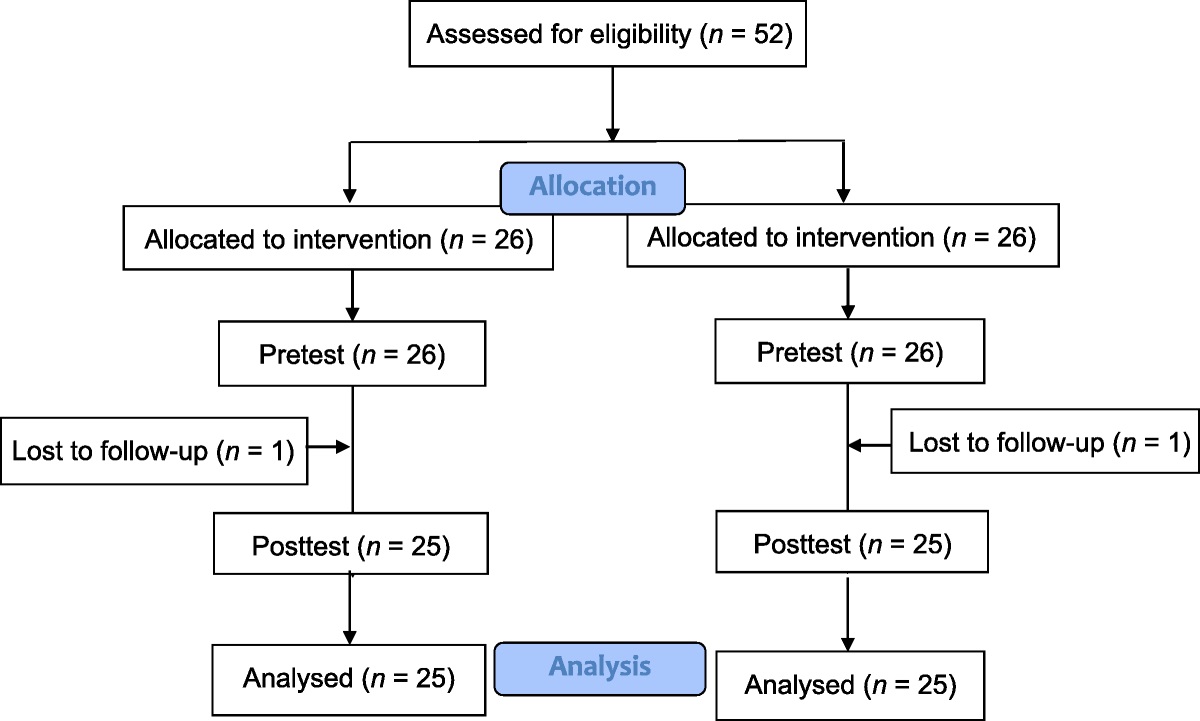
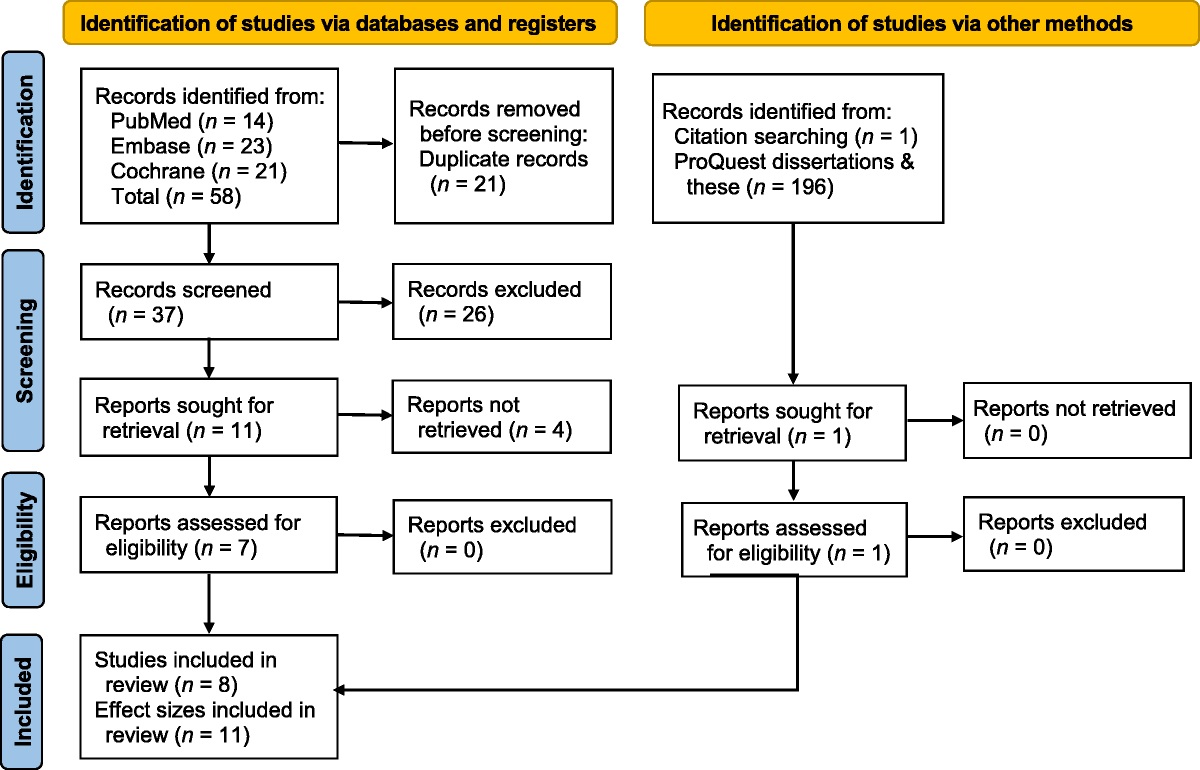
Results Study Selection and InclusionThe initial search yielded 58 articles (Figure 1). After screening of the titles and abstracts, 21 duplicates and 26 irrelevant articles were excluded, and seven articles were retained for full-text assessment. Also, 196 potentially eligible theses and dissertations and one additional study (Tseng et al., 2014) were identified using the citation search. Finally, eight RCTs (Biçer & Taşci, 2022; Y. C. Cho & Tsay, 2004; Chun & Park, 2016; Eğlence et al., 2013; Sabouhi et al., 2013; Tsay, 2004; Tsay et al., 2004; Tseng et al., 2014) were included in the meta-analysis. Three studies (Sabouhi et al., 2013; Tsay, 2004; Tsay et al., 2004) used a three-arm study design, resulting in 11 effect sizes for the data analysis.
 Figure 1:
Figure 1: Flow Diagram of Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020Note. Three 3-arm studies of the eight included studies using two different controls resulting in 11 effect sizes.
Characteristics of the Included StudiesSeven hundred twenty-five participants with a mean age of 57.78 years were included in this analysis (Table 1). In terms of the included trials, four were conducted in Taiwan (with six effect sizes; Y. C. Cho & Tsay, 2004; Tsay, 2004; Tsay et al., 2004; Tseng et al., 2014), one was conducted in South Korea (Chun & Park, 2016), one was conducted in Iran (with two effect sizes; Sabouhi et al., 2013), and two were conducted in Turkey (Biçer & Taşci, 2022; Eğlence et al., 2013). All of the trials included patients who had been receiving regular hemodialysis for at least 3 months. Most of the trials (eight effect sizes) used Sanyinjiao (SP6), Yongquan (K1), and Zusanli (ST36) as treatment acupoints (Y. C. Cho & Tsay, 2004; Eğlence et al., 2013; Sabouhi et al., 2013; Tsay, 2004; Tsay et al., 2004); four trials (six effect sizes) used Yanglingquan (GB34; Eğlence et al., 2013; Sabouhi et al., 2013; Tsay, 2004; Tsay et al., 2004) as a treatment acupoint; and three trials (four effect sizes) used Shenmen (HT7/TF4) as an additional treatment acupoint (Chun & Park, 2016; Sabouhi et al., 2013; Tseng et al., 2014). In four of the trials, the participants reported feelings of soreness, numbness, heaviness, distension, or warmth during the acupressure intervention (Y. C. Cho & Tsay, 2004; Tsay, 2004; Tsay et al., 2004; Tseng et al., 2014). All of the interventions were conducted during hemodialysis treatment by trained researchers. In five of the trials, the acupressure interventions were conducted with the use of assistive equipment, with Biçer and Taşci (2022) using an electrostimulation device, Y. C. Cho and Tsay (2004) using finger pads, Chun and Park (2016) using acupoint stickers, Eğlence et al. (2013) using a transcutaneous electrical nerve stimulation pen, and Tsay et al. (2004) comparing the efficacy of acupressure performed by fingers and by a transcutaneous electrical acupoint stimulation device. In most of the studies (nine effect sizes; Biçer & Taşci, 2022; Y. C. Cho & Tsay, 2004; Eğlence et al., 2013; Sabouhi et al., 2013; Tsay, 2004; Tsay et al., 2004), posthemodialysis fatigue level was measured using the Piper Fatigue Scale (Piper et al., 1998), whereas one study (Chun & Park, 2016) used the Multidimensional Fatigue Scale (Tack, 1991), and another study (Tseng et al., 2014) used the Novel Fatigue Scale for Hemodialysis Patients (C.-C. Lin et al., 2006). Five RCTs with eight effect sizes reported the results of four subscales of Piper Fatigue Scale, including behavioral, emotional, sensory, and cognitive fatigue (Biçer & Taşci, 2022; Eğlence et al., 2013; Sabouhi et al., 2013; Tsay, 2004; Tsay et al., 2004).
Table 1 - Characteristics of Included Studies (N = 11) Study, Year Country Population Age (Years) Female (%) Sample Size Acupoints Frequency Control Equipment/Operator Complication Outcome Instrument Biçer & Taşci (2022) Turkey Hemodialysis patients who experienced hypotension during hemodialysis 64.9 60 135 Neiguan (P6) Each session lasted for 1 hour, 3 times/week, for 1 month Placebo Electrostimulation device/researcher NR PFS Y. C. Cho et al. (2004) Taiwan Hemodialysis patients 49.51 56.9 58 Sanyinjiao (SP6), Taixi (KI3), Yungchuan (K1), Zusanli (ST36) Each point 3 minutes, total of 12 minutes/day, 3 days/week, for over 4 weeks Usual care Finger pads/researcher NR PFS Chun & Park (2016) Korea Hemodialysis patients 62.41 53.7 41 Adrenal gland (TG2p), brain stem (between AT3.4 and AH12i), Chuiqian (LO4), earlobe (LO5–LO9), endocrine (CO18), Fengxi (SF1.2i), Helix 1 (HX9), Helix 2 (HX10), large intestine (CO7), Sanjiao (CO17), Shenmen (TF4), subcortex (AT4), sympathetic (AH6a), Zhen (AT3) Once a week for 3 days, for 10 weeks Usual care Acupoint stickers/researcher NR MFS Eǧlence et al. (2013) Turkey Hemodialysis patients 54.2 48.30 118 Sanyinjiao (SP6), Yanglingquan (GB34), Yungchuan (K1), Zusanli (ST36) Each point 3 minutes, total of 12 minutes/day, 3 times/week, for 1 month Usual care TENS acupuncture pen/researcher NR PFS Sabouhi et al. (2013)a Iran Hemodialysis patients 54 43.75 48 Sanyinjiao (SP6), Shenmen (HT7), Shenshu (BL23), Yanglingquan (GB34), Yongquan (K1), Zusanli (ST36) Each session lasted for 20 minutes, of which 2 minutes was for stroking of the acupoints and the rest of the time (18 minutes) was for acupressure of the determined six acupoints (3 minutes for each acupoint), 3 days/week for 4 weeks Usual care Finger/researcher NR PFS Sabouhi et al. (2013)b Iran Hemodialysis patients 54.7 43.75 48 Sanyinjiao (SP6), Shenmen (HT7), Shenshu (BL23), Yanglingquan (GB34), Yongquan (K1), Zusanli (ST36) Each session lasted for 20 minutes, of which 2 minutes was for stroking of the acupoints and the rest of the time (18 minutes) was for acupressure of the determined six acupoints (3 minutes for each acupoint), 3 days/week for 4 weeks Sham acupressure Finger/researcher NR PFS Tsay (2004)a Taiwan Hemodialysis patients 56.94 66 53 Sanyingjao (SP6), Yanglingquan (GB34), Yungchuan (K1), Zusanli (ST36) 12 minutes of acupoints massage (3 minutes/acupoint). One course lasted for 3 days per week, for 4 weeks. Usual care Finger/researcher NR PFS Tsay (2004)b Taiwan Hemodialysis patients 59.38 66 53 Sanyingjao (SP6), Yanglingquan (GB34), Yungchuan (K1), Zusanli (ST36) 12 minutes of acupoints massage (3 minutes/acupoint). One course lasted for 3 days per week, for 4 weeks. Sham acupressure Finger/researcher NR PFS Tsay et al. (2004)a Taiwan Hemodialysis patients 58.16 66 52 Sanyingjao (SP6), Yanglingquan (GB34), Yungchuan (K1), Zusanli (ST36) 12 minutes of acupressure (3 minutes/acupoint), 3 times per week, for 4 weeks Usual care Finger/researcher NR PFS Tsay et al. (2004)b Taiwan Hemodialysis patients 58.16 66 54 Sanyingjao (SP6), Yanglingquan (GB34), Yungchuan (K1), Zusanli (ST36) 12 minutes of acupressure or TEAS (3 minutes/acupoint), 3 times per week, for 4 weeks TEAS Finger or TEAS/researcher NR PFS Tseng et al. (2014) Taiwan Hemodialysis patients NR 67.69 65 Neiguan (PC6), Shenmen (HT7), Tianzhu (BL10), Yongquan (K1) Each point press for 5 seconds and then relax for 1 second, continue for 3 minutes, three times a week, 15 minutes each time, for 4 weeks Usual care Finger/researcher NR Novel Fatigue Scale for hemodialysis patientNote. Studies with a and b were three-arm studies using two different controls. NR = no report; PFS = Piper Fatigue Scale; MFS = Multidimensional Fatigue Scale; TENS = Transcutaneous Electrical Nerve Stimulation; TEAS = Transcutaneous Electrical Acupoint Stimulation.
The overall judgment of “some concerns” was reported in four studies (six effect sizes; Biçer & Taşci, 2022; Sabouhi et al., 2013; Tsay, 2004; Tseng et al., 2014), whereas that of “high risk of bias” was reported in the other four studies (five effect sizes; Y. C. Cho & Tsay, 2004; Chun & Park, 2016; Eğlence et al., 2013; Tsay et al., 2004). Regarding the overall risk of bias, the randomization process and deviations from the intended interventions were the two main causes of the “high risk of bias” and “some concerns.” Two of the trials did not conceal the allocation adequately (Chun & Park, 2016; Eğlence et al., 2013), and three may have applied inappropriate analysis methodologies (Y. C. Cho & Tsay, 2004; Chun & Park, 2016; Tsay et al., 2004), leading to the determinations that these four trials (five effect sizes) were “high risk of bias.” The “some concerns” rating in the other four trials (six effect sizes) was associated with the lack of information about the allocation sequence and the concealment of the allocation (Biçer & Taşci, 2022; Sabouhi et al., 2013; Tsay, 2004; Tseng et al., 2014; Table 2).
Table 2 - Risk of Methodological Bias Score of the StudiesNote. Studies with a and b were three-arm studies using two different controls. + = low risk; − = high risk; ? = some concerns.
Acupressure was found to reduce general fatigue significantly with a large effect size of −0.78 (95% CI [−1.09, −0.48], p < .01), as shown in Figure 2. Substantial heterogeneity was identified among the included studies using Cochran's Q statistics and I2 values (Q = 36.23, p < .01, I2 = 72.40%). Moderator and meta-regression analyses were performed to explore the factors contributing to significant between-study heterogeneity.
 Figure 2-A:
Figure 2-A: Forest Plots of Effect Sizes for Studies Measuring (A) General Fatigue, (B) Behavioral Fatigue, (C) Emotional Fatigue, (D) Sensory Fatigue, and (E) Cognitive FatigueNote. Studies with a and b were three-arm studies using two different controls.
 Figure 2-B:
Figure 2-B: Forest Plots of Effect Sizes for Studies Measuring (A) General Fatigue, (B) Behavioral Fatigue, (C) Emotional Fatigue, (D) Sensory Fatigue, and (E) Cognitive FatigueNote. Studies with a and b were three-arm studies using two different controls.
The pooled effect sizes (g) for the behavioral, emotional, sensory, and cognitive domains of fatigue were −0.51 (95% CI [−0.82, −0.20], p < .01), −0.51 (95% CI [−0.73, −0.28], p < .01), −0.72 (95% CI [−1.04, −0.39], p < .01), and −0.41 (95% CI [−0.66, −0.17], p < .01), respectively, indicating acupressure significantly relieved different aspects of posthemodialysis fatigue. Furthermore, the results of Cochran's Q (20.83, 11.12, 22.18, and 13.24, respectively; p = .004, .134, .002, and .066, respectively) and I2 statistics (66.39%, 37.03%, 68.44%, and 47.13%, respectively) indicated the presence of significant heterogeneity across the included studies.
Moderator and Meta-Regression AnalysesThe results of the moderator and meta-regression analyses are listed in Table 3. The fatigue-reduction effect in studies using the Shenmen acupoint was larger than in those that did not use this acupoint (p < .01). Also, the ratio of female patients correlated positively with the fatigue reduction effect (g = 0.04, p < .01). Notably, the effect of acupressure on fatigue reduction was not found to be moderated by the use of any device (p = .99), indicating that acupressure may be performed effectively using fingers (g = −0.79) or special equipment (g = −0.79). No statistically significant difference in study quality was observed between the “high risk of bias” and “some concerns” studies (p = .65).
Table 3 - Moderator and Meta-Regression Analyses (N = 11) Parameter n Effect Size (g) 95% CI p Meta-regression Age a 10 0.02 [−0.06, 0.10] .610 Female 11 0.04 [0.01, 0.07] .008 Moderator analyses Operation approaches .990 By finger 7 −0.79 [−1.22, −0.35] Others b 4 −0.79 [−1.27, −0.31] Control group c .780 Usual care 8 −0.68 [−0.86, −0.51] Acupoint stimulation 2 −0.87 [−1.31, −0.44] Yanglingquan acupoint selection .660 No 4 −0.87 [−1.29, −0.45] Yes 7 −0.73 [−1.17, −0.29] Shenmen acupoint selection .006 No 7 −0.48 [−0.66, −0.30] Yes 4 −1.42 [−2.06, −0.78] Risk of bias .650 Some concern 6 −0.87 [−1.32, −0.42] High risk 5 −0.72 [−1.18, −0.25]Note. CI = confidence interval.
aTseng et al. (2014) did not provide the mean age of the participants, so it was excluded from the meta-regression analysis of age.b Electrostimulation device, finger pads, transcutaneous electrical nerve stimulation acupuncture pen, acupoint stickers, or transcutaneous electrical acupoint stimulation.
c Only Tsay (2004) provided massage as the control arm, which could not be classified as either usual care or acupoint stimulation. Therefore, it was excluded from the moderator analysis.The results of the Egger regression analyses showed no significant publication bias for behavioral fatigue (p = .15), emotional fatigue (p = .46), sensory fatigue (p = .11), or cognitive fatigue (p = .08). However, significant publication bias was found for general fatigue (p = .01).
DiscussionThe beneficial effects of acupressure in terms of reducing general, physical, and mental fatigue in patients with cancer as well as in healthy people have been demonstrated in prior systematic review and meta-analysis studies (Hsieh et al., 2021; Song et al., 2015). This meta-analysis of randomized patients receiving hemodialysis (n = 725) supports that acupressure effectively alleviates general fatigue as well as subdomains of fatigue, including behavior, emotion, sensory, and cognitive. The results provide additional evidence for the beneficial effects of acupressure in terms of alleviating fatigue in patients receiving hemodialysis and suggest the clinical practicability of using acupressure treatments on patients with various diseases.
However, although the beneficial effects were found, the exact mechanisms underlying the effects of acupressure on fatigue remain unclear. Changes in brain neurochemistry and connectivity during acupressure interventions is one potential mechanism. Harris et al. (2017) found stimulating both relaxing and stimulating acupoints affects functional connectivity in the brain, suggesting the potential involvement of neural mechanisms in fatigue relief.
Within the framework of traditional Chinese medicine, the human body contains numerous acupoints, each of which corresponds to a specific organ or body part. By stimulating a specific acupoint, the flow of qi along the associated meridian may be regulated, effectively treating the associated disease (J. Lin et al., 2022). The findings of the moderator analyses in this study indicate that both finger stimulation and device-based stimulation achieved comparable effects in terms of fatigue mitigation. This suggests that the approach to stimulation rather than the method of operation is the crucial factor in achieving therapeutic effects through acupressure. Further studies are needed to explore the impacts of variables such as acupressure strength, intensity, and duration on fatigue reduction.
The findings of the moderator analysis suggest that targeting the Shenmen acupoint (in addition to the Sanyinjiao, Yongquan, and Zusanli acupoints) significantly increases the fatigue-reduction effect of acupressure. Cheung et al. (2015) found the decline in brain activity after stimulating the Shenmen acupoint, which is associated with reduced arousal, suggests Shenmen acupoint stimulation may promote sleep. Strong scientific evidence supports that increasing total sleep time reduces the symptoms of fatigue (Dean, 2022; Mantua et al., 2019), which may explain the beneficial effect of Shenmen acupoint selection on fatigue alleviation in patients receiving hemodialysis. However, the question remains regarding the direction of the effect between sleep improvement and fatigue mitigation.
LimitationsThis study was affected by several limitations. First, half of the included studies were judged as “high risk” or “some concerns” of bias, which may threaten the internal validity of the findings. Second, all of the included trials were conducted in East Asia or the Middle East, which may limit the generalizability of the findings to other geographic regions and populations. Lastly, publication bias was identified for the included studies that investigated general fatigue. Thus, the findings of this study should be interpreted with appropriate caution.
Implications for Clinical PracticeThe etiology of fatigue following hemodialysis is unclear, and few nonpharmacological interventions for reducing fatigue are currently available. The findings of this systematic review and meta-analysis suggest acupressure to be a cost-effective and easy-to-perform therapeutic intervention for alleviating different aspects of fatigue in patients receiving hemodialysis. The main practical implication is that the effect of acupressure on fatigue reduction is significant only when the Shenmen acupoint is targeted along with other acupoints (i.e., Sanyinjiao, Yongquan, and Zusanli). Furthermore, acupressure may be effectively performed with either fingers or special equipment. Healthcare providers should teach patients receiving hemodialysis who complain of fatigue to use acupressure therapy to alleviate their fatigue
Comments (0)