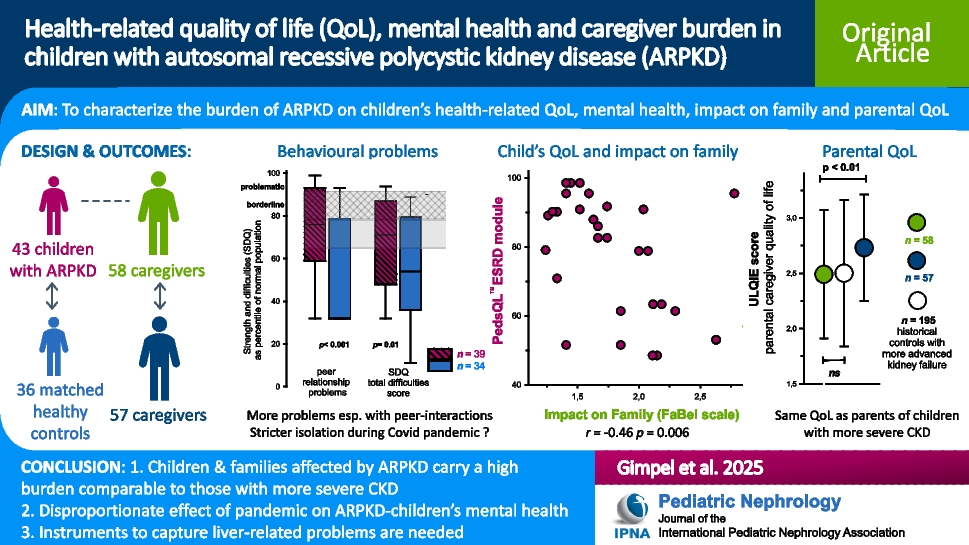
This study presents the first disease-specific data on the impact of ARPKD on pediatric patients’ health-related quality of life (hrQOL), mental health and caregiver burden. We chose the PedsQL®ESRD instrument to capture hrQOL, the SDQ questionnaire to screen for emotional and behavioural problems, the ULQIE to assess parental QOL and the FaBel score to quantify the impact of the disease on the entire family because they have all been used in the same cultural context before and enabled comparison to historical pediatric controls who were either healthy or affected by other chronic kidney diseases. In terms of psychometric properties in the ARPKD population, the internal consistency, as measured by Cronbach’s α, was very good for the self-reported PedsQL®ESRD, ULQIE and FaBel scores. The PedsQL®ESRD proxy score was slightly less consistent, but still good, confirming previous reports of the local-language PedsQL®ESRD versions from Belgium [33], Brazil [34] and Malaysia [35]. The consistencies of ULQIE and FaBel in this study were also similar to those found in the initial studies [29, 30]. The SDQ score achieved only a good Cronbach α for the proxy version and a fair value in the self-reported version; however, this is consistent with its properties in large samples of adolescents from Germany and around the world [25, 27], suggesting that consistent concepts are captured in this subpopulation compared to the originally intended ones. The significant differences between SDQ and ULQIE scores in affected families versus contemporary healthy controls (see Fig. 1 and Fig. 2a) support their discriminant validity in reflecting the mental burden of living with and caring for a child with ARPKD. Regarding content validity and face validity, the kidney disease–specific PedsQL®ESRD questionnaire performed well in reflecting severity of kidney disease (see Fig. 4). However, the absence of a correlation between PedsQL®ESRD score and abdominal circumference (or its z-score) reflects the fact that PedsQL®ESRD is not designed to cover symptoms of liver enlargement and dysfunction, such as abdominal discomfort, bloating, poor appetite, gastrointestinal bleeding or itching, which are a special feature of ARPKD compared to other causes of childhood CKD. Unfortunately, there are no instruments available yet for capturing symptoms of children with portal hypertension. In our view therefore, the development of an ARPKD-specific patient-reported outcome measure to capture symptoms is needed, if future clinical trials in ARPKD are to reflect patient burden adequately.
In terms of documenting the burden of ARPKD on children, the hrQOL PedsQL®ESRD total scores of children on dialysis and after kidney transplantation were in a similar range to those previously reported for children with other causes of kidney failure [4]. The better PedsQL®ESRD scores post-transplant compared to on dialysis found here (see Table 3) confirmed a number of previous studies using self-reporting (see [4] for a meta-analysis), and proxy reports [7]. Fewer studies have reported PedsQL®ESRD in children with CKD prior to kidney failure, but those found here were higher than in children with CKD from Brazil and Thailand [36, 37]. The FaBel score indicated that the impact of ARPKD on family life was at a similar level as that of other chronic pediatric diseases (epilepsy, diabetes and childhood cancer) in the past [29]. While some aspects of caregiver burden caused by a child’s chronic disease are probably similar between these diseases (such as giving regular medications, supervision restrictions in diet, time spent for medical appointments), the greater scores of ARPKD parents in the subdomain of worries about the future may be either a pandemic effect or reflect the fact that the future necessity of a kidney transplant weighs heavy on parents even at an early stage of impaired kidney function [6]. Both impact on family (FaBel) and parental quality of life (ULQIE) total scores were similar to a group of parents of children with more severe kidney disease from 2010 [3], suggesting a more severe impact of ARPKD compared to other types of kidney failure. The emotional and behavioural screening questionnaire SDQ revealed a significantly increased total difficulties score compared to contemporary healthy controls (Fig. 1). This is consistent with previous reports in children with mixed cause CKD without controls which reported mental health difficulties using the SDQ [5, 38, 39] or other assessment tools [36]. However, a study with a large national control sample did not find a higher prevalence of a formal diagnosis of depression, anxiety or attention-deficit and hyperactivity disorder (ADHD) in children with CKD [40]. However, in that study, there was a poor correlation of a screening questionnaire on depressive symptoms and a formal diagnosis of depression. We speculate that the more ‘tangible’ effects of CKD distract healthcare professionals from mental and behavioural problems. The high correlation of total PedsQL®ESRD score and total SDQ score in our group should alert the clinician to be aware of the increased risk of psychosocial problems in children with more pronounced symptoms of their kidney disease. We found a high correlation of the child’s disease severity on parental stress levels and parental well-being, that is in line with recent studies using other instruments [8, 9, 36]. Perinatal presentation of ARPKD was a particular risk factor for higher caregiver burden (ULQIE and FaBel), but less for the child’s current hrQOL or emotional well-being. Overall, we could demonstrate that children with ARPKD carry a similar if not greater burden of kidney disease–related reduction in QOL and associated psychological problems, as well as burden on family life and parental reduction in QOL, than families affected by other chronic kidney diseases.
The most significant extra-renal risk factor for reduced hrQOL, emotional problems and higher caregiver burden was a co-existing developmental delay of the child. In multivariate analysis, it remained significant after adjusting for treatment modality. Interestingly, in the large Korean KNOW-Ped cohort study, both developmental delay and multi-organ involvement were also significant risk factors for mental health problems and adjustment problems [41] in children with CKD. While developmental delay is as an important factor for parental stress in both pre-school and school-age children [42, 43], it is also known to aggravate other parenting stressors such as poverty, history of immigration [42] or pandemic restrictions [44] and appears to be mediated by a lack of interactive engagement behaviours of the child [45]. As developmental delay was never due to an additional disease, but always secondary to a complication of ARPKD such as prematurity or severe hypotensive episodes, we emphasize the need for high-quality medical care for these children in order to avoid complications of ARPKD.
Our study opened the unplanned opportunity to study the interaction of the stress for children and their families of coping with CKD in addition to pandemic restrictions. It was notable that our healthy contemporary controls had higher SDQ problem scores than historical controls, especially for emotional symptoms, conduct problems and hyperactivity/inattention, which was most likely attributable to the pandemic. A large longitudinal population-based study in German children also showed a significant increase in the mean SDQ from pre-pandemic levels during 2020 and 2021 [12, 46], which only slightly decreased in autumn 2021 and 2022 [47]. This was true for all subdomains of the SDQ but most pronounced for hyperactivity symptoms, followed closely by conduct and peer problems and still noticeable for emotional problems [12]. Notably, in that cohort, SDQ scores recovered more slowly than a hrQOL measure as the pandemic progressed [47]. A study from Brazil in adolescents with a wider range of immunocompromising chronic diseases also showed increased SDQ during the pandemic, but not over and above that of contemporary healthy controls [19]. However, in our German ARPKD cohort, peer relationship problems were significantly increased above those of contemporary controls, which may reflect the fact that children with ARPKD were more strictly shielded from social contacts than healthy children during the pandemic, resulting in greater social isolation. A longitudinal study of children with nephrotic syndrome suggested that during the pandemic levels of fatigue rose [48]. However, from our data, it seems that fatigue was not increased more than in contemporary controls, especially in self-report (see Table S3). Despite the fact that parental quality of life (ULQIE scores) was lower in caregivers of children with ARPKD compared to contemporary caregivers of healthy children (who also bore special strains during the pandemic [11]), the subjective impact of the pandemic was rated lower by parents in ARPKD families than by contemporary control parents. Potentially, this reflects an increased focus on coping with the disease as a protective factor against the subjective feeling of being overwhelmed by contact restrictions and a global event out of their control.
The study was limited by the fact that no instruments are available to record symptoms of portal hypertension in children and the difficulty of quantifying hepatic morbidity in early disease, both because less reliable biomarkers are available and disease progression is less linear than decline in kidney function. Participant numbers were small compared to studies in healthy children, because of the very low incidence of ARPKD and the added difficulties of performing personal interviews during a time of fluctuating contact restrictions. Recruitment via treating physicians and self-help organisations may lead to a bias towards patients with better outcomes and/or more articulate families. Feasibility in terms of completion time was not assessed, but this has been reported for the PedsQL®ESRD and SDQ previously [22, 35, 49, 50].
In summary, ARPKD causes significantly impaired hrQOL, emotional and behavioural problems and caregiver burden, which were equal to, if not greater than, that of historical cohorts of children with all-cause kidney failure. More problems with peer interactions may be due to more stringent shielding of chronically ill children from social contacts during the COVID pandemic compared to healthy children. Additional developmental delay was a risk factor for both physical and mental well-being of the child, parental QOL and the disease’s impact on the family. For future clinical trials in ARPKD, better quantification of liver-related symptoms is needed.



Comments (0)