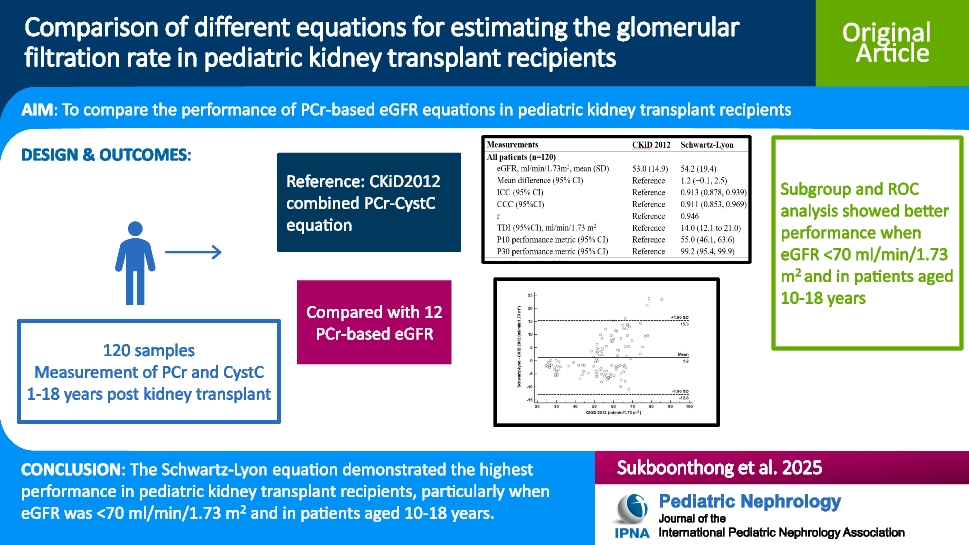
This study comprehensively evaluated the performance of 12 PCr-based eGFR equations in pediatric kidney transplant recipients, using the CKiD 2012 combined PCr–CystC equation as the reference standard. Among the tested equations, the Schwartz–Lyon formula showed the highest overall performance, with excellent ICC (0.913), CCC (0.911), TDI (14.0 mL/min/1.73 m2), and the highest P30 performance metric (99.2%). Its reliability was particularly notable in patients with eGFR < 70 mL/min/1.73 m2 and those aged 10–18 years. The U25, FAS–height, and Bedside Schwartz equations demonstrated comparable performance and serve as reasonable alternatives.
Recent guidelines for renal function monitoring in solid organ transplant recipients highlight the importance of selecting an appropriate GFR estimation method tailored to the patient’s physiological characteristics [17]. The KDIGO 2024 guidelines reinforce the role of the combined PCr-CystC-based formula in clinical decision-making, particularly when the PCr-based formula alone is less reliable [17]. Pizzo et al. assessed mGFR in 45 pediatric kidney transplant recipients using several equations, including the CKiD 2012 and U25 combined PCr–CystC formulas, and found both performed similarly and ranked among the best estimators [31]. In our study, which used the CKiD 2012 combined equation as the reference, the U25 combined equation also demonstrated excellent agreement (ICC = 0.993, CCC = 0.990, TDI = 3.9 mL/min/1.73 m2, P30 = 100%), supporting its potential as an alternative equation when CystC is available.
Our study showed that the Schwartz–Lyon equation had the best overall performance, particularly in patients with eGFR < 70 mL/min/1.73 m2 and those aged 10–18 years. The U25, FAS–height, and Bedside Schwartz also performed comparably and support previous findings on the value of pediatric-specific formulas for estimating GFR in this population [7, 9, 10, 19]. Compared with previous pediatric studies, the findings align closely with those of de Souza et al. [7], who reported that the Schwartz–Lyon equation demonstrated good performance with respect to mGFR, particularly at lower GFR levels (mGFR < 60 mL/min/1.73 m2), with high P30 accuracy rates (97–98%) and better reliability than other PCr-based equations. Additionally, Papez et al. evaluated eGFR estimation in a Hispanic-dominant pediatric kidney transplant population and reported that the Bedside Schwartz equation demonstrated the highest correlations with mGFR using iothalamate clearance [9]. A previous study by Tsampalieros et al. compared the Bedside Schwartz eGFR with the CKiD 2009 combined with the PCr-CysC formula in pediatric kidney transplant recipients and reported that the Bedside Schwartz formula overestimated the GFR, with a mean bias of 1.09 mL/min/1.73 m2 [32]. However, they did not include the Schwartz–Lyon equation. A previous Canadian study by Alkandari et al. found that the modified Schwartz and FAS-age equations demonstrated better bias and P30 accuracy in pediatric kidney transplant recipients [10], although FAS-height was not assessed. In contrast, our study demonstrated superior performance of FAS-height over FAS-age. This discrepancy may reflect population-specific growth patterns. In our Thai cohort, post-transplant growth retardation is common, making age a less reliable proxy for body size. As FAS-height incorporates actual stature, it may better capture renal function in this population. Conversely, the Canadian cohort may have had growth patterns more aligned with the original European derivation cohort of FAS-age, contributing to its better performance in that setting.
A previous study conducted by de Souza et al. analyzed the performance of different eGFR equations in pediatric kidney transplant recipients and assessed their ability to correctly classify renal dysfunction using AUC analysis. They reported that the Schwartz–Lyon and Bedside Schwartz AUCs were 0.97 and 0.96, respectively, for detecting an mGFR < 60 mL/min/1.73 m2 [7]. Consistent with our findings, this study reinforces the need for equation-specific eGFR thresholds, as identified by our ROC analysis (< 70 mL/min/1.73 m2 for Schwartz–Lyon, U25, and FAS-height and < 60 mL/min/1.73 m2 or Bedside Schwartz). Additionally, a Canadian study by Alkandari et al. found that the modified Schwartz performed best in children aged 5–15 years. In our study, the Bedside Schwartz showed better performance in those aged 10–18 years. These results highlight the importance of selecting eGFR equations with high classification accuracy, particularly in populations at risk of developing allograft dysfunction.
This study has several strengths. First, our study comprehensively compared several PCr-based eGFR equations. This comprehensive comparison provides substantial advantages over studies that evaluate only a limited number of equations. Second, this study focused on a unique clinical population of pediatric kidney transplant recipients receiving adult donor kidneys. This focus provides valuable insights into the performance of eGFR equations tailored to the unique physiological and clinical characteristics of these patients, thereby filling a critical gap in nephrology research. Third, the application of advanced statistical analyses, including Bland‒Altman plots, ICCs, and performance metrics such as P10 and P30 performance metrics, ensures a thorough assessment of each eGFR formula’s reliability and agreement with the reference standard. These methods are widely recognized for their effectiveness in method comparison studies, enhancing the credibility of the results. Fourth, ROC analysis was used to define eGFR thresholds at which each equation maintains optimal accuracy, and subgroup analyses by age were performed. This approach enhances clinical applicability by offering more precise guidance for renal function assessment in pediatric kidney transplant recipients.
There are some limitations in this study. First, although the sample size calculation indicated the need for at least 120 samples to demonstrate a significant difference [7], this study included only 23 patients because of the limited number of transplant recipients at our center during the study period. However, each individual measurement remained independent and did not exert any influence on the others. Second, there is a lack of direct mGFR assessments to confirm the absolute accuracy of the eGFR equations. While eGFR equations are widely used and practical for clinical application, they may not always precisely reflect the true GFR. Consequently, our study relies on comparative analyses between different eGFR equations rather than direct GFR measurements. Third, while corticosteroids may affect CystC levels, a prior study in pediatric kidney transplant recipients revealed no significant correlation between CystC levels and prednisolone use [33]. Furthermore, this study included only patients receiving low-dose prednisolone (< 0.5 mg/kg/day), which may have minimized any potential impact on CystC levels. Fourth, although timing post-transplant may influence the performance of eGFR equations, our dataset included only four eGFR measurements obtained within the first 3 months after transplantation. Due to this limited sample size, we were unable to perform a dedicated subgroup analysis for this early post-kidney transplant period. Fifth, the CKiD 2012 equation was developed in children with mostly stage 3 or higher CKD and may not fully reflect transplant recipients with near-normal GFR [13]. In our study, most equations performed better in the < 75 mL/min/1.73 m2 group. Similarly, a recent study noted reduced accuracy of eGFR equations at higher GFR levels, highlighting the need for improved models for children with preserved kidney function [34]. Future research should involve larger, multicenter studies—including patients in the early post-kidney transplant period and incorporating direct GFR measurements to increase the validity and reliability of kidney function assessment methods in pediatric kidney transplant recipients.
In conclusion, the Schwartz–Lyon equation demonstrated the highest performance in estimating the eGFR in pediatric kidney transplant recipients, particularly when eGFR was < 70 mL/min/1.73 m2 and in patients aged 10–18 years, and should be considered the preferred equation in this population when CystC is not available. Notably, the U25 combined PCr-CystC equation showed the best overall agreement of the reference CKiD 2012 combined equation and may be preferred in clinical settings when CystC measurement is feasible. The U25, FAS–height, and Bedside Schwartz equations demonstrated comparable performance and serve as reasonable alternatives. These findings reinforce the importance of selecting appropriate eGFR estimation methods tailored to the physiology of pediatric kidney transplant patients.



Comments (0)