
Remember me



A total of 405 patients underwent robotic SBRT from April 2021 to September 2023 and were divided into two categories as follows: (1) 5-fraction SBRT (n = 309, 76%), and (2) 3-fraction boost post pelvic nodal irradiation (n = 96, 34%). There were obvious differences in cancer and treatment characteristics given the population of patients. The entire cohort had a median age of 70 years. After separating the cohorts into two groups, we observed significant difference when comparing age, with the 5-fraction consisting of younger patients on average (69 vs. 72 years, p < 0.001). Unsurprisingly, PSA levels in the 3-fraction cohort were substantially higher than in the 5-fraction (11.9 vs. 4.6 ng/mL, p < 0.001). Similarly, given the preponderance of high-risk disease in the 3-fraction cohort, more aggressive grade grouping characteristics were evident (p < 0.001). The use of rectal spacers was common in both cohorts but significantly more frequent in the 5-fraction group than in the 3-fraction group, precluding them from spacer placement. Finally, when assessing ADT administration, see the majority of patients in the 3-fraction boost cohort received ADT (84 vs. 35%, p < 0.001) (Table 1).
Table 1 Patient and tumor characteristics in the 3- and 5-fraction patient cohortsFiducial characteristicsFiducial placement characteristics were essentially the same between groups with both 3- and 5-fraction cohorts having a median fiducial count of 4 (range: 2 to 6 and 2 to 5, respectively), with no significant difference in the mean count between cohorts (p = 0.38). In our study, a minimum of 4 gold fiducials were implanted in all patients with up to 6 fiducials implanted. There was a significantly increased median time from fiducial placement to first SBRT fraction within the 3-fraction cohort (82 vs. 42 days, p < 0.001), which reflects the delayed treatment initiation due to the administration of neoadjuvant ADT and pelvic RT in this high-risk population. Due to the often-every-other day schedule for the SBRT boost cases, the median time from SBRT start to finish for both cohorts was 5 days. However, not surprisingly, the mean duration of treatment for the 5-fraction cohort was significantly longer (7.44 versus 4.63 days, p < 0.001).
Fiducial trackingOverall, within the 3-fraction cohort, tracking was either perfect or had attrition of only one fiducial 100%, 97.9%, and 99% of the time from fraction 1 to 3, respectively. Similarly, within the 5-fraction cohort, tracking was either perfect or had attrition of only one fiducial 97.1%, 96.8%, 97.1%, 95.1%, and 95.8% of the time from fraction 1 to 5, respectively. Thus, given the median number of fiducials placed for both 3-and 5-fraction cohorts was at least four, this loss of one fiducial had no intra-fractional motion management significance from a clinical standpoint given the ability to track translations and rotations achievable with 3 fiducials. Interestingly, on average, attrition of a single fiducial was slightly higher in the 3- versus the 5- fraction cohort (64% vs. 59%).
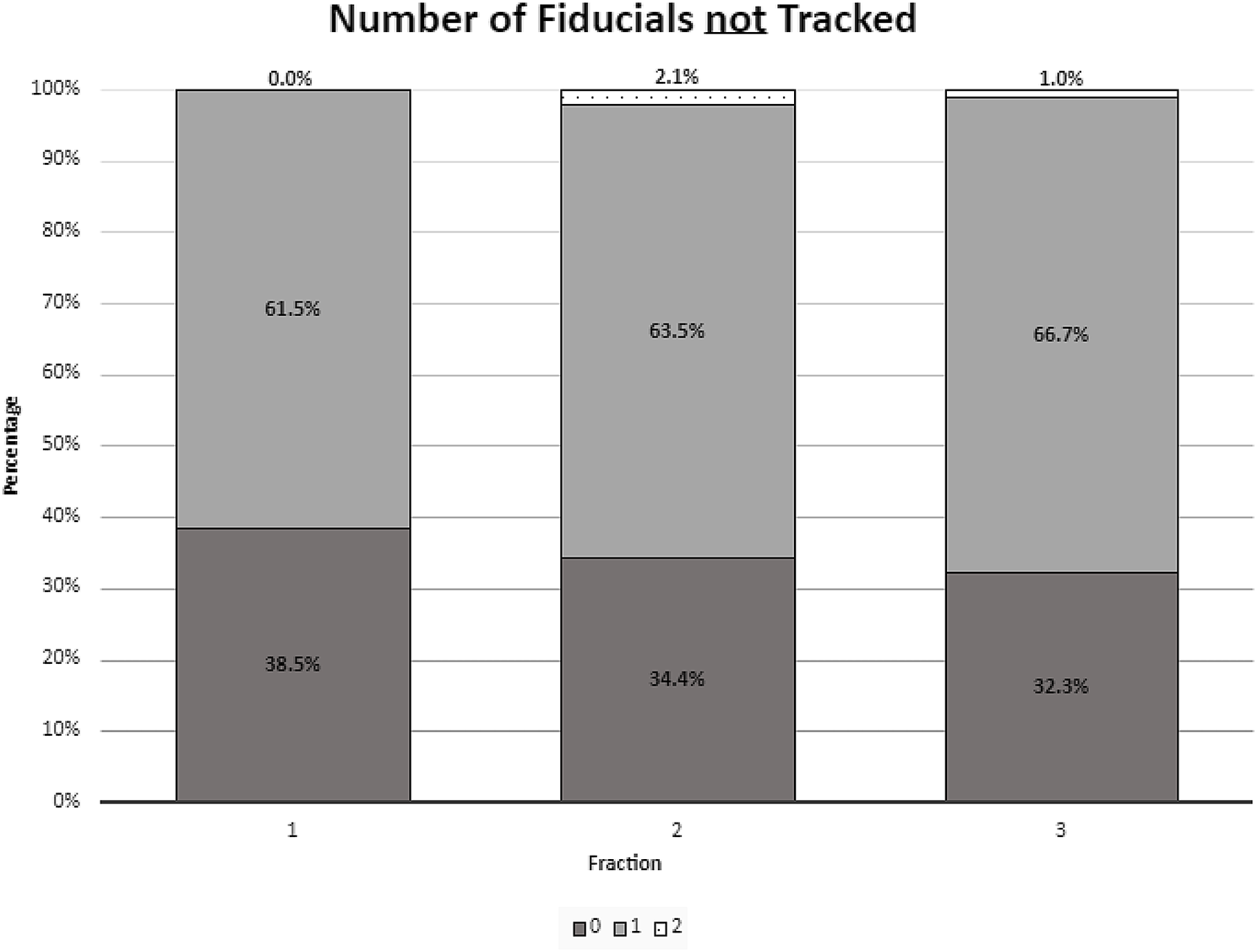
We investigated the temporal change in fiducial tracking within the same 3- and 5-fraction cohorts categorized by loss of 0, 1, or 2 fiducials for a given treatment fraction. Overall, there was no significant tracking loss over the 3-fraction boost treatment regimen that followed nodal treatment (p = 0.63) (Fig. 1). In contrast, with over 5 treatment fractions, there was a significant loss of fiducial tracking fidelity as demonstrated by progressive loss of a single tracked fiducial (Fig. 2). Of note, the 3-fraction regimen displayed higher rates of loss of a single fiducial tracked (61.7–66.7%) relative to the 5-fraction regimen (44.0–67.3%). As such, although the 5-fraction regimen displayed progressive loss of a single fiducial, the single lost fiducial was fixed from the outset for the 3-fraction regimen. In both 3- and 5- fraction cases, a second lost fiducial was a rare event that occurred ≤ 5% of the time.
Fig. 1
Fiducials not tracked for the 3 fraction cohort
Fig. 2
Fiducials not tracked within the 5 fraction cohort
We then analyzed the volatility of the fiducial tracking pattern, that is, which specific fiducial set was tracked for a given fraction across the full SBRT boost course for a given patient. We observed significantly more volatility over the 5-fraction cohort relative to the 3-fraction boost (2.4 vs. 0.0, p < 0.001), indicating that the optimal fiducial tracking set was more variable fraction to fraction in the 5-fraction cohort versus the 3-fraction cohort.
Analysis of fiducial tracking associations with pre-treatment clinical factors was performed in three fashions to explore (1) fiducial tracking volatility, (2) temporal pattern changes from the first to last treatment fractions, and (3) deviations from the most commonly tracked fiducial set regardless of temporal associations during the fractional delivery. There were no statistically significant associations between tracking using either analysis method or volatility for the following parameters: time from fiducial placement to SBRT, CTV, or QOD vs. daily SBRT delivery (Table 2). However, use of concomitant ADT approached significance when analyzing median volatility in the 5- versus the 3-fraction cohort (1.12 versus 2.24, p < 0.058). Of note, for all patients undergoing SBRT, our institutional practice is to allow for a 1 to 3-month neoadjuvant ADT course prior to initiating SBRT. Clinical associations with fiducial tracking are displayed in Table 2.
Table 2 Associations between pre-treatment factors and fiducial tracking parameters (volatility, temporal pattern, and deviation from ideal tracking) in the 3-fraction and 5-fraction SBRT cohorts
Comments (0)