A 66-year-old female presented to her primary care provider with a chief complaint of unintentional 35-pound weight loss. She had a medical history inclusive of advanced Parkinson’s disease treated with carbidopa/levodopa 25–250 mg thrice per day and a 47-pack year smoking history. Her weight loss workup included a chest x-ray, which visualized a hazy left upper lobe (LUL) infiltrate. A subsequent diagnostic CT scan characterized the infiltrate as a peripherally located 2.4 cm spiculated nodule. A CT-guided biopsy successfully sampled adenocarcinoma. An 18-flurodeoxyglucose positron emission tomography (PET) scan identified mild tracer avidity in the LUL lesion (maximum standardized uptake value of 2.5) without evidence of disease elsewhere. Magnetic resonance imaging (MRI) did not identify intracranial metastatic disease. She was diagnosed with American Joint Committee on Cancer (AJCC) 8th edition cT1cN0M0 stage 1A3 lung adenocarcinoma.
Her pulmonary function tests were within normal limits, and a cardiothoracic surgeon assessed that she could be a candidate for surgery, but she elected against surgery. Local radiation oncologists indicated she could not be safely treated with SBRT due to her Parkinsonian tremors. She consulted our service for a second opinion, and we likewise observed that she could not voluntarily control her tremors long enough to receive RT. However, we discussed definitive SBRT to the LUL adenocarcinoma delivered as 34 Gy in a single fraction with anesthesia services to facilitate immobilization. Moreover, because the patient lived many hours from our institution, we conceived a direct-to-unit, single-visit RT course wherein an initial beam arrangement would be drafted on a recent diagnostic CT and adapted at treatment using the Ethos platform (Varian Medical Systems, Palo Alto, CA). On the day of treatment, conscious sedation and paralysis with propofol and rocuronium were induced, and online adaptation began.
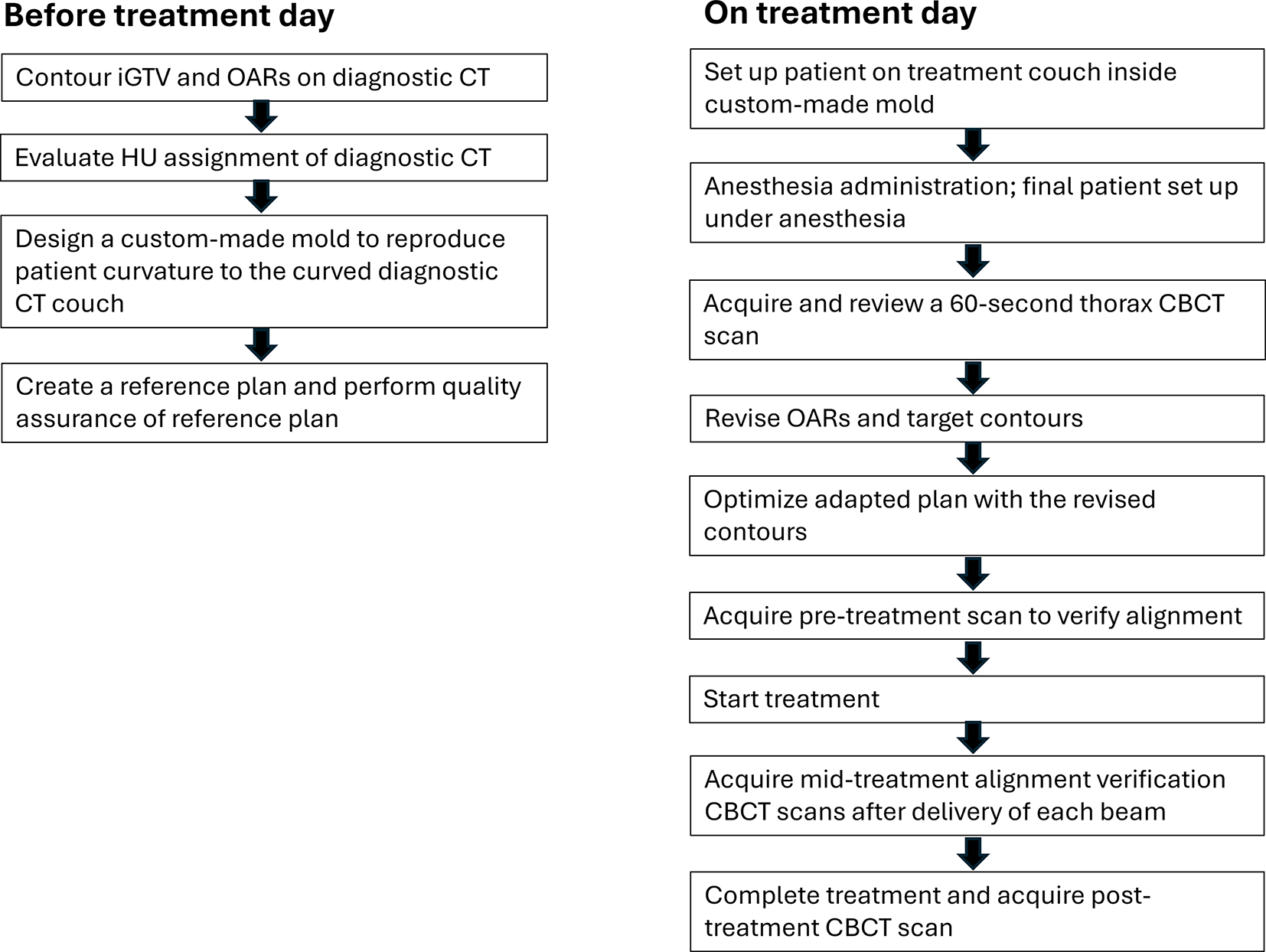
Direct-to-unit workflowDiagnostic-scan based pre-planning
Figure 1 illustrates the workflow for this case of direct-to-unit ART. A treatment plan was created on a diagnostic CT acquired in a clinic close to the patient’s home on a curved couch-top without patient-specific immobilization and with a high-pitch acquisition that obfuscated possible lesion motion (Fig. 2). The patient’s arms were positioned above her head for this scan. Given that online adaptation on our current Ethos platform performs dose calculation on a synthetic CT (sCT) derived from deformably warping the diagnostic CT, a custom foam-based mold (Fig. 3) was fabricated based on the diagnostic CT to approximately replicate positioning on the diagnostic CT and limit large deformations that could produce an inaccurate sCT. To assess the appropriateness of dose calculation on the sCT obtained from the diagnostic scan, voxel-by-voxel material assignments were qualitatively reviewed based on an institutional Hounsfield Unit (HU)-to-mass density calibration curve for our CT scanners. An initial internal gross tumor volume (iGTV) was contoured on the diagnostic scan. A planning target volume (PTV) was generated as a 5 mm radial and 8 mm superior/inferior expansion of the iGTV (Fig. 2). Organs at risk (OARs) including chest wall, great vessels, esophagus, bronchial tree, and heart were contoured on the axial slices within three centimeters of the PTV.
An initial “reference plan” was generated based on the diagnostic CT. Custom rule-based structures were created to limit dose spill into mediastinal anatomy and ensure a centralized hot spot in the iGTV with rapid dose fall-off. An automatic normalization of the plan to meet priority 1 goals for OARs was implemented in the optimization. In the other words, the treatment planning system always normalized to meet the P1 objectives after optimization, if necessary. No normalization was applied based on target coverage criteria. The objectives and dose constraints for OARs and targets that were used in the optimization are shown in Table 1. A beam geometry of four partial coplanar arcs was specified based on target laterality and to provide well-defined intervals for mid-treatment imaging.
Table 1 Plan objectives for OARs and target for the reference plan (calculated on diagnostic CT), scheduled and adapted plans (calculated on deformed diagnostic CT), and the treated adapted plan re-calculated on 60-second thorax CBCTOnline adaptive treatment planning & delivery
The patient was positioned on the treatment table in the foam mold under anesthesia. A 60- second CBCT acquisition was performed through the lungs. The iGTV contour, which was initially defined on diagnostic CT imaging for creating an initial plan, was rigidly aligned to the lesion as visualized on the CBCT. The attending radiation oncologist manually adjusted the iGTV contour on the CBCT to conservatively contain the apparent motion envelope. As a 60-second CBCT captures all breathing phases, the envelope of the moving GTV (iGTV)– including blurry boundaries– was assumed to estimate the internal target volume (ITV). Given the patient’s regular and controlled breathing with rate of 14 breaths per minute while under anesthesia and limited motion for this tumor in the upper lobe, we were confident in the delineation of iGTV as an estimate of ITV. For a quantitative comparison of target delineation on initial plan (diagnostic scan) and adaptive plan (CBCT), the iGTV volumes were 7.2 cc and 7.9 cc for diagnostic CT and treatment CBCT, respectively, with 0.1 cm shift in their center of mass.
After contouring, a reference plan was calculated on the patient’s anatomy-of-the-day and deemed the “scheduled plan.” Next, the Ethos treatment planning system (TPS) re-optimized the plan considering the patient’s anatomy and generated an adapted plan. Optimization was completed in five and a half minutes. The constraints and target coverage metrics for the scheduled and adapted plans are shown in Table 1. Although no OAR constraints were violated, target coverage improved by approximately 5% with the adapted plan, and therefore this plan was selected for treatment.
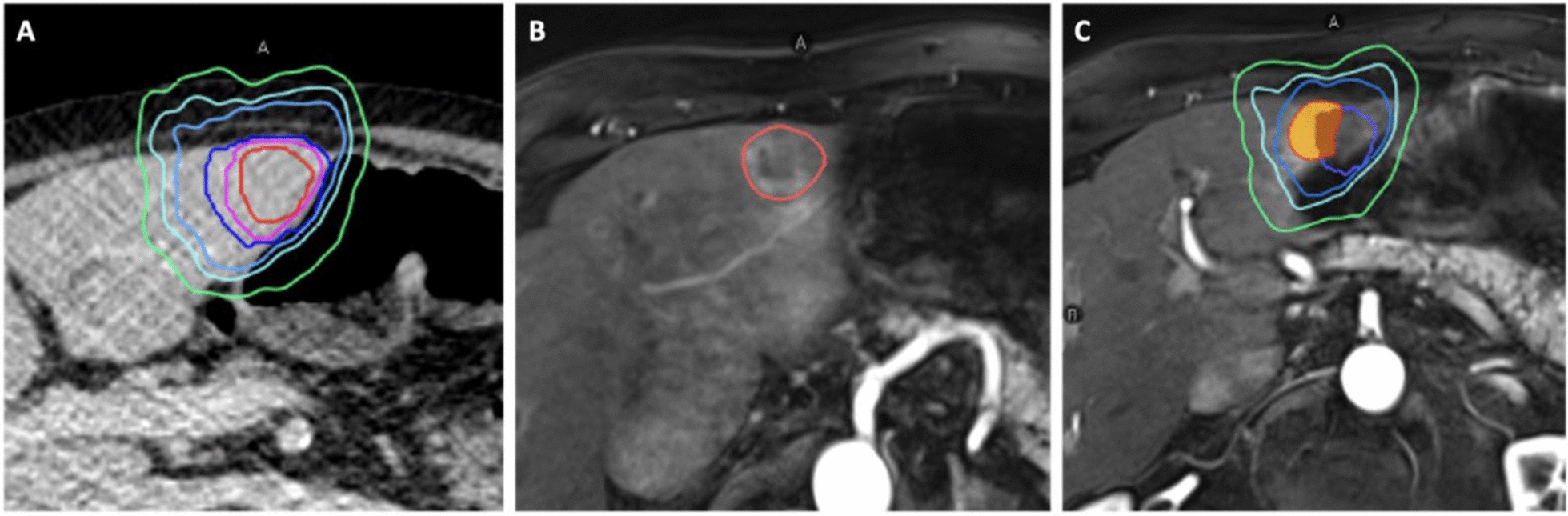
A pre-treatment 60-second CBCT was acquired for final alignment. Verification CBCTs were acquired after each delivered field. The time from initial CBCT to treatment completion was 63 minutes. Subsequently the adapted plan was imported to Eclipse and re-calculated on the CBCT. Figure 4 shows the comparison of isodoses lines and DVHs for target coverage calculated on sCT and CBCT scans. The patient tolerated the treatment well and had no adverse effects from the sedation.




Comments (0)