This retrospective study collected data from patients treated in our centre over a period of nearly ten years, for liver metastases or HCC with SBRT delivered in more than 4 fractions due to OAR proximity. Despite a reduction in the total prescribed dose, which resulted in lower BED10 and EQD2 values, LC remains satisfactory.
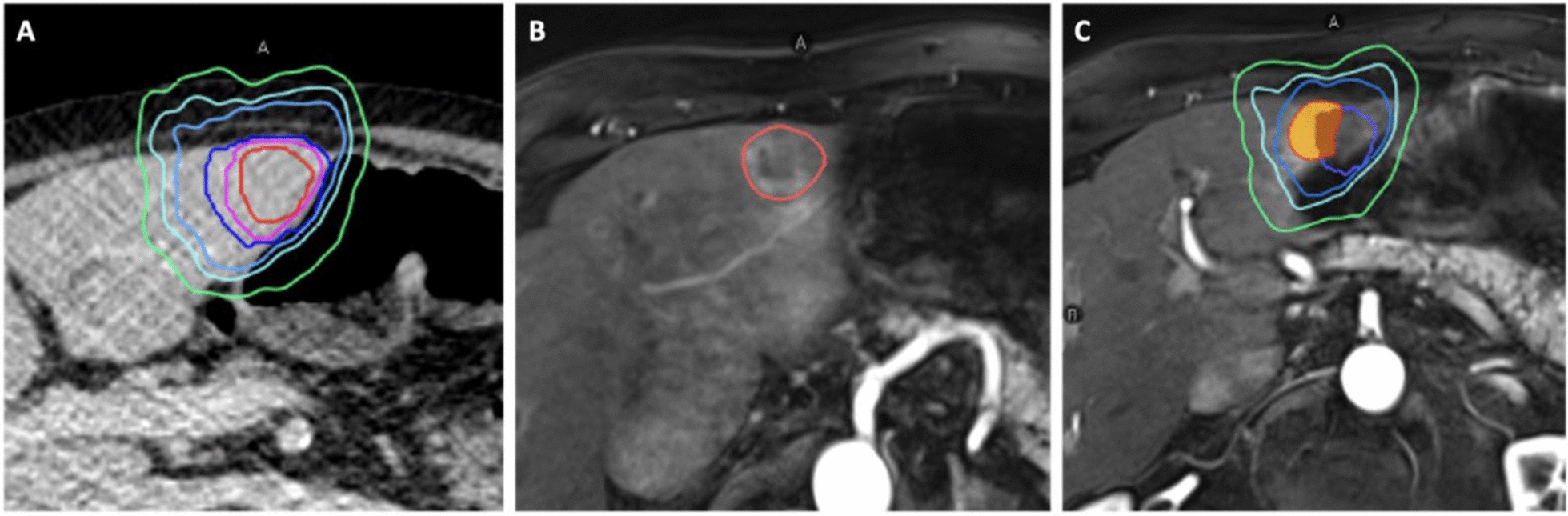
This is the first study to accurately delineate liver recurrence volumes on follow-up imaging. This delineation enabled us to compare recurrence volumes with treatment isodoses and thus better define and describe LR.
Our study showed a LC rate of 87.5% for the treated lesions, based on the number of recurrences sharing more than 80% of their volume with the V80% isodose. This LC rate decreases to 71.9% when considering recurrences sharing more than 20% volume with the V80% isodose.
Previous studies have assessed lesion response on follow-up imaging but without volume delineation. Our results are in accordance with these studies. Kwon et al. found an initial lesion response followed by an in-field progression at 2.5 years of 28.6% after SBRT treatment in 3 fractions [14], while Joo et al. found 32% in-field recurrence at 3 years following delivery in 3 to 4 fractions [15]. The slightly lower LC in our study can be explained by the lower BED10 and EQD2 in our study due to the delivery of treatments in more than 4 fractions.
However, the definition of in-field recurrence was not the same in our study as in the two earlier studies. Indeed, Kwon et al. defined in-field response as “target lesion response within the irradiated field”, while Joo et al. defined local failure as a “new nodular or irregular enhancing lesion in the previous tumour site", excluding new out-of-field liver metastases.
Our study found a LC rate of 64% based on 36% of LR overlapping with the initial volumes and isodose treatment, regardless of the percentage of shared volume.
One meta-analysis published in 2019 indicated a 2-year LC rate of 83% for both HCC and liver metastases when treated with SBRT delivered in 3 or 4 fractions, BED10 > 93 Gy and EQD2 > 78 Gy [22]. Another literature review on HCC treated with SBRT delivered in 4 to 6 fractions reported a LC rate ranging from 73 to 98% at 3 years, with BED10 between 51 and 180 Gy and EQD2 between 42 and 150 Gy [23]. For liver metastases LC rate ranged between 67 and 95% in prospective studies and from 58 to 100% in retrospective studies, with the most frequently reported BED10 at 112.5 Gy [24].
Our LC rate is slightly lower than that observed in these trials, which can be attributed to the dose reduction necessary to comply with the dose constraints for the OAR in our patient population. We reported BED10 values ranging from 52.5 to 100 Gy, with a most commonly prescribed dose of 59 Gy, and EQD2 values ranging from 43.75 to 93.33 Gy, with most commonly prescribed dose of 49.58 Gy.
Also, the definition of LC in published papers is not always clear or precise: are we considering in-field progression or marginal progression? What is the definition of "in-field" progression: a lesion in the same liver segment or sharing volume with the initial treatment volumes? This may have influenced the interpretation of the results, and comparisons between different studies should be made cautiously.
As described in the literature [3, 8,9,10], we observed that lower BED10, for HCC or liver metastases, was associated with lower LC and recurrence occurring within the initial treatment isodose volume.
While some studies have reported a potential association between tumour volume and LC at various cut-off points [3, 14] we found no such association in our study, possibly due to the majority of lesions studied being smaller than 5 cm.
According to the departmental protocol, all patients treated during the recruitment period were scheduled to receive standard treatment delivered in 3 fractions. Only when this failed to comply with the dosimetric constraints due to OAR, the delivery in 4 or more fractions was then planned to reach compliance and maintain PTV coverage as high as possible.
Even at the lower prescription dose, we found some non-compliance with these constraints due to extreme proximity between the target lesion and the OAR, especially in the duodenum or stomach. Fortunately, these non-compliances were minimal and resulted in no significant toxicity compared to published data.
There are limitations to this work. First this study remains a retrospective cohort with a small number of patients and a heterogeneous population including HCC and liver metastasis regardless of the initial histology.
Moreover, image fusion between planning CT and MRI or CT of recurrence was not always easy, with changes in liver parenchyma anatomy due to cirrhosis, intercurrent local treatment or different respiratory phase. The volumes delineated on CT scans are also less suitable than those delineated on MRI. To increase the validity of our data, image fusion and recurrence volumes were reviewed by two radiation oncologists and all recurrences were identified by a radiologist. If more than one recurrence was found on the same follow-up image, we chose to delineate the closest recurrence to account for the worst-case scenario.
Three patients were treated without fiducial markers using Spine tracking prior to 2015, due to medical contraindications or tumour locations deemed close enough to the vertebrae. These patients did not benefit from PTV margin adjustments in contrast to the other patients treated with fiducial markers. However, these patients did not appear to have a consequentially higher recurrence rate than the others: two patients showed no recurrence during their follow-up, while one patient experienced a marginal recurrence at the 80% isodose.
Given the heterogeneity of the dose delivered in SBRT, it is reasonable to hypothesise that maintaining a higher ablative dose within the PTV may, even with lower coverage, allow satisfactory and in particular safe treatment of the target lesion, thanks to a steep dose gradient sparing the OAR. In a secondary analysis of the SABR-COMET trial, Van Oirschot et al. [13] suggested that PTV coverage was not associated with improved OS or LC. These findings were confirmed in a recent secondary analysis of the SABR-5 trial [25] in oligometastatic patients with prioritisation of OAR in a larger cohort.
Further prospective data are now needed to determine whether prioritising a high ablative BED10/EQD2 is more beneficial than ensuring maximum coverage of the PTV at all costs. This is essential to ensure satisfactory control of the target lesion while sparing the nearby OAR.




Comments (0)