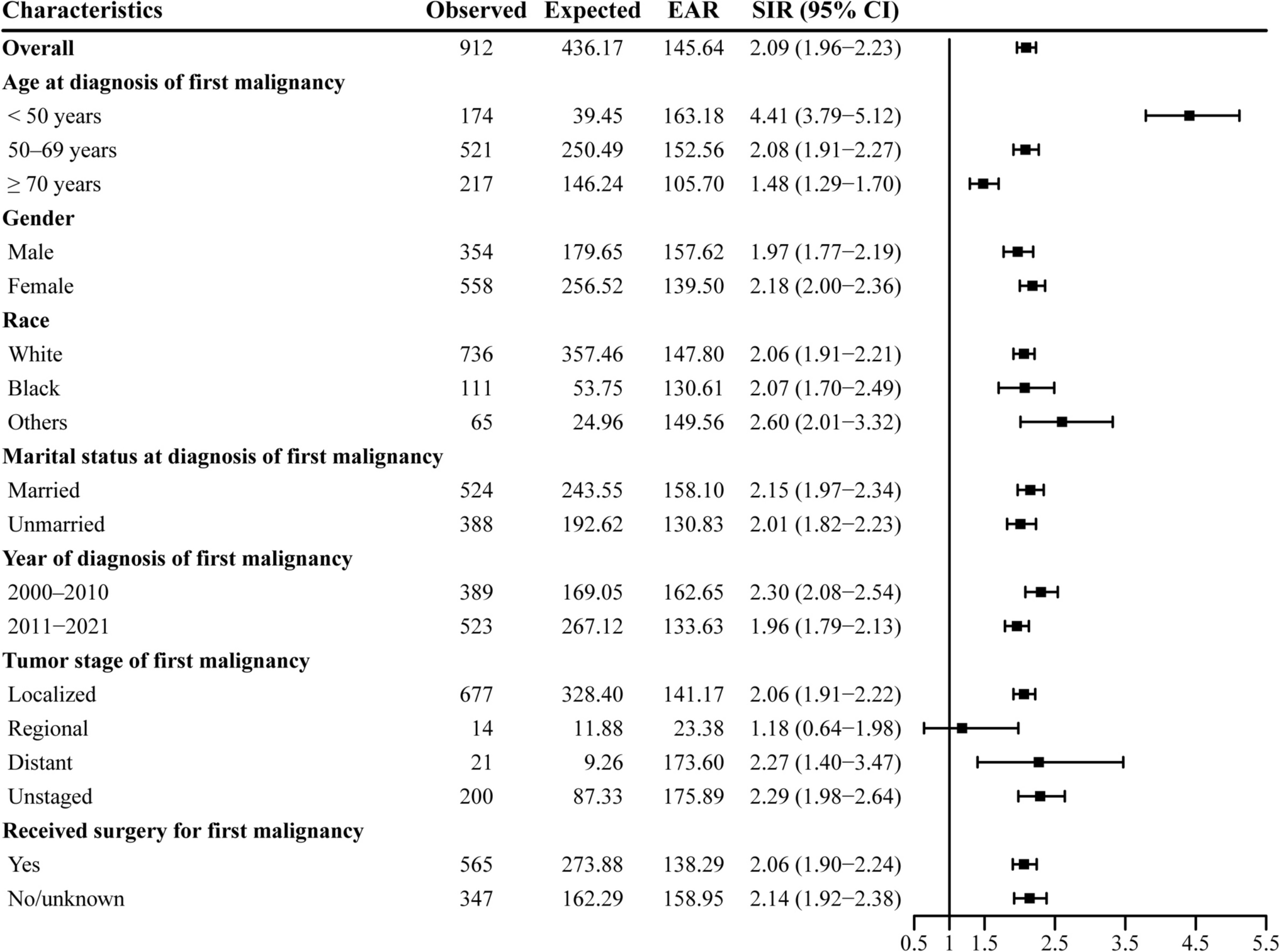
This large-scale cohort study examines the relationship between the initial primary malignancy and the subsequent development of SPMs among survivors of G-NETs in the United States from 2000 to 2021. To our knowledge, this is the first systematic investigation of the risk of SPMs in G-NET survivors. The cohort comprised 5,072 G-NET patients, of whom 912 (18.0%) were diagnosed with an SPM during the follow-up period. The median interval between the diagnosis of the first and second malignancy was 34.3 months. Overall, survivors of G-NETs demonstrated a 109% higher risk of developing SPMs relative to the general U.S. population, with an EAR of 145.64 cases per 10,000 person-years. The most commonly observed SPMs included cancers of the stomach, small intestine, thyroid, and hepatobiliary system. Our results can guide clinicians in identifying high-risk groups among G-NET survivors who may benefit from more intensive monitoring and early intervention.
A study conducted at a tertiary referral center in the Netherlands investigated the incidence of SPMs in patients diagnosed with gastroenteropancreatic neuroendocrine tumors (GEP-NETs). The cohort included 459 patients who were diagnosed between 2000 and 2009, with 67 individuals (13.7%) subsequently diagnosed with a SPM. The findings indicated that synchronous SPMs—defined as those occurring within 6 months before or after the GEP-NET diagnosis—were significantly more prevalent in this population, particularly colorectal cancers. Despite this, the authors concluded that routine screening for SPMs in GEP-NET patients is not justified, as the elevated risk was confined to synchronous malignancies, rather than a broader increased risk for subsequent cancers [18]. In contrast, a more extensive, population-based analysis utilizing data from the SEER registries assessed the risk of SPMs in NET patients from 2000 to 2016. Among 58,596 patients, 4612 (7.9%) developed a SPM. This study identified a statistically significant increase in the risk of SPMs in NET patients, with an SIR of 1.35 (95% CI 1.31–1.39). The cumulative five-year incidence of SPMs varied by the primary site of the NET, ranging from 3.8% for pancreatic NETs to 5.9% for gastrointestinal NETs [17]. Further investigations focusing on patients with pancreatic and gastrointestinal NETs corroborated these findings, revealing that individuals with these tumor types are at a considerably higher risk of developing additional malignancies [19].
Our analysis of SPMs in relation to key patient characteristics provides valuable insights into risk stratification and the optimization of surveillance protocols. The risk of developing SPMs decreased progressively with increasing age, which suggests a potential age-dependent protective effect against the development of additional malignancies. This trend could be attributed to several underlying factors. Firstly, the shorter life expectancy typical of older individuals may reduce the likelihood of developing a second malignancy within the time frame preceding death [20]. Additionally, age-related immune system changes, such as immunosenescence, could impair the body’s capacity to detect and eliminate malignant cells, thereby attenuating cancer progression and reducing the occurrence of SPMs [21, 22]. Moreover, older patients are less likely to undergo routine cancer screenings, which may further contribute to the observed decline in SPM incidence with increasing age. For instance, a study conducted in Taiwan involving 1350 newly diagnosed NET patients revealed an increased risk of second malignancies, particularly among individuals aged 70 years or older [23]. In clinical practice, the management of older patients with G-NETs requires a nuanced approach. Clinicians must balance the potential benefits of intensive SPM surveillance with the limitations imposed by reduced life expectancy. Such considerations are essential for developing personalized follow-up strategies that integrate both chronological age and overall health status, thereby optimizing patient care and ensuring resource-efficient monitoring. It is also important to consider that the SEER database has a higher proportion of older individuals. This demographic characteristic of the database could potentially influence the observed decrease in SPM risk with advancing age. Specifically, the lower representation of younger patients in the SEER data might limit our ability to fully characterize the risk of SPMs in this population.
As time progresses, the risk of developing a SPM decreases; however, even after 10 years, the risk remains elevated, indicating that the initial diagnosis of G-NETs and the long-term effects of the disease may continue to predispose patients to subsequent malignancies. One potential explanation for this sustained risk is that individuals with a history of G-NET may experience persistent immunological alterations or chronic inflammation, which could contribute to a heightened susceptibility to new malignancies [24, 25]. Additionally, the prolonged elevated risk may reflect underlying genetic predispositions or pre-existing conditions that increase the likelihood of developing multiple cancers. For instance, patients with inherited cancer syndromes or a family history of malignancy may be more prone to the development of secondary malignancies [26, 27]. Furthermore, the genetic mutations or tumor suppressor gene alterations that initially drove G-NET tumorigenesis may also play a role in the pathogenesis of secondary cancers, suggesting a shared molecular pathway between primary and secondary malignancies. These findings highlight the need for ongoing surveillance in patients with G-NETs, as the elevated risk of secondary malignancies persists beyond 10 years and may remain a significant concern throughout the patient’s lifetime.
Our study indicates that while women may exhibit a higher SIR for SPMs, the EAR is greater in men. This disparity may be attributed to gender differences in lifestyle factors that predispose individuals to certain cancers. Men are more likely to engage in behaviors such as smoking, alcohol consumption, and obesity, all of which are known to increase the risk of various malignancies [28, 29]. These lifestyle factors may partly explain the higher EAR observed in males. Smoking, for example, is a well-established risk factor for numerous cancers, including those of the oral cavity, pharynx, and lungs. The higher prevalence of smoking among men may account for the elevated risk of oral and pharyngeal cancers observed exclusively in male patients. Similarly, alcohol consumption is a known contributor to the development of liver cancer, which may further elevate the risk in males. Both sexes demonstrated increased risks for malignancies of the gastric, small intestine, hepatobiliary system, pancreas, and thyroid, suggesting that the biological mechanisms underlying G-NETs might predispose patients to these specific malignancies. These malignancies, often associated with the gastrointestinal and endocrine systems, may share common pathways of tumorigenesis with G-NETs. For instance, neuroendocrine tumors are known to secrete bioactive amines that can influence cellular function and growth in other tissues, potentially heightening susceptibility to secondary malignancies [30, 31].
Racial disparities were detected in our study. White patients were found to have a risk comparable to that of Black patients, suggesting that while genetic factors may contribute, variations in the SIRs for SPMs across racial groups could also be influenced by disparities in healthcare access and treatment. Notably, White patients exhibited the highest risk for stomach cancer compared to other racial groups. This disparity may be attributed to specific lifestyle factors, such as dietary habits, smoking prevalence, and alcohol consumption, which have been linked to higher incidences of stomach cancer in certain populations.
This cohort study offers several notable strengths, including a large sample size, an extended follow-up period, and a population-based design, all of which enhance the external validity of the results, allowing for generalization to the wider U.S. population. Nonetheless, certain limitations must be acknowledged. First, while the SEER database provides robust population-level data, it lacks granular details on socioeconomic status, environmental exposures (e.g., smoking, alcohol use, dietary habits), and genetic predispositions (e.g., hereditary syndromes like MEN1), which may confound the observed risks of SPMs. Second, treatment specifics, such as chemotherapy regimens, radiation doses, or prolonged use of somatostatin analogs, were unavailable, limiting our ability to assess their potential role in SPM development. Third, while the substantial sample size and extended follow-up duration provide valuable insights, the relatively low frequency of the events under study resulted in wide confidence intervals. Finally, the assumption of a two-month latency period between cancer diagnoses may have contributed to an overestimation of the SPM incidence. Therefore, caution is warranted in the interpretation of these findings.
Over the next 5 years, we anticipate transformative shifts in this field. Personalized risk prediction models incorporating genetic, clinical, and lifestyle data will likely become standard tools for guiding SPM surveillance. Advances in liquid biopsy technologies may enable early detection of secondary malignancies through circulating tumor DNA or neuroendocrine-specific biomarkers. Additionally, immunotherapy trials targeting immune checkpoints (e.g., PD-L1 inhibitors) in G-NETs could reveal whether these therapies mitigate SPM risk by modulating the tumor microenvironment.


Comments (0)