Although the response of patients to treatment has dramatically improved in recent years with the advent of precision therapies for lung cancer, such as immunotherapy and targeted therapy, the 5-year survival rate is still only 21% [21]. Early screening, diagnosis, and timely treatment are the keys to a good prognosis for lung cancer patients [22]. Clinically, the presence of small nodules in a patient’s lungs on CT imaging is critical in determining early lung cancer [23]. Nonetheless, not all lung nodules are malignant, and in a large-scale study of CT screening for lung cancer, it was found that about 49% of cancers screened for may be overdiagnosed [24, 25]. In recent years, the prevalence of pulmonary nodules identified through chest CT scans conducted during routine medical care has risen significantly. Consequently, the effective management of both incidental and screen-detected nodules has emerged as a critical public health concern [26]. Therefore, improving the ability to recognize and predict benign and malignant lung nodules is vital to treating lung cancer.
At present, the primary challenge in managing lung nodules lies in accurately identifying high-risk nodules with potential malignancy and stratifying patients into distinct risk categories to inform subsequent management strategies [26]. In the NELSON trial, it was observed that participants with nodules measuring < 5 mm in diameter exhibited a low probability of developing lung cancer [27, 28]. Conversely, those with nodules ranging from 5 to 10 mm demonstrated a moderate probability, while nodules ≥ 10 mm were associated with a significantly increased likelihood of lung cancer development [27, 28]. In accordance with the Fleischner guidelines, distinct management strategies are necessitated for solid and subsolid pulmonary nodules. Specifically, for solid pulmonary nodules > 8 mm in size, tissue sampling is advised. [29]. In Japan, the protocol for LDCT lung cancer screening advises follow-up evaluations at intervals of 3, 6, 12, 24, 36, 48, and 60 months for nodules with an overall mean diameter of < 15 mm and a solid component measuring < 8 mm in diameter [30]. The [Chinese Expert Consensus on the Diagnosis and Treatment of Pulmonary Nodules (2024)] delineates 18 consensus points, underscoring the critical importance of early diagnosis and intervention. It recommends specific screening ages for high-risk populations, clarifies the definition of lung nodules and the methodologies for their assessment, and advocates for the integration of artificial intelligence to enhance diagnostic accuracy [31]. Ye et al. proposed for the first time an adjustment of the criteria for a positive result in chest CT screening for pure ground-glass nodules of the lung in a Chinese population [32]. They suggested that the criteria should be raised from 6 to 8 mm and that only pure ground-glass nodules with a diameter of 8 mm and above should require management of lung nodules [32].
Liquid biopsy, as a non-invasive approach, has received widespread attention for its ease of repeated analysis and its ability to monitor tumor recurrence, metastasis, and response to treatment in real-time [33]. With the rapid development of molecular techniques, circulating tumor cells, circulating tumor DNA, circulating cell-free RNA, circulating cell-free DNA, and extracellular vesicles show potential clinical value in the diagnosis, treatment, and prognosis of lung cancer, but the low concentration of them in the blood results in low sensitivity of liquid biopsies [33]. Recently, Chen et al. developed an epigenetic biomarker model based on circulating ribosomes that is particularly effective in identifying high-risk lung nodules [34]. For the first time, MD Anderson researchers found that the 4MP was helpful for lung cancer risk prediction, with a higher AUC value for the 4MP + smoking model than the smoking-based risk prediction model (0.83 vs. 0.73) [19]. Afterward, researchers analyzed the performance of 4MP in distinguishing lung cancer from benign lung nodules [35]. The researchers found that the 4MP + nodules size model had a higher AUC (0.895) than the model based on nodule size alone (AUC was 0.860) or 4MP (AUC was 0.757), and in the independent validation cohort, the AUC of 4MP was 0.87 [35]. In the past two years, to step forward to determine the role of 4MP in lung cancer, researchers explored the lung cancer risk prediction performance of the 4MP + PLCOm2012 model and found the 4MP can be used for lung cancer risk assessment, with AUC values of 0.80 for 4MP alone detection and 0.85 for the combined 4MP + PLCOm2012 model for sera from cases collected within 1-year preceding diagnosis [36]. Moreover, Vykoukal et al. analyzed the predictive performance of 4MP in distinguishing lung cancer patients from controls and found an AUC value of 0.80 for 4MP, whereas the AUC value for 4MP + miR-210-3p + miR-320a-3p + miR-21-5p was 0.81 [37]. In 2024, MD Anderson Cancer Center researchers analyzed repeated measurements of 4MP in pre-diagnostic serum from 2483 ever-smoker participants [38]. They improved the performance of 4MP in the early detection of lung cancer using a parametric empirical Bayes algorithm [38]. However, most of these studies have investigated clinical diagnoses in Western populations. Lung cancer types, environmental factors, and genetic susceptibility are different between Western and Asian populations [39]. Yao et al. found that 4MP combined with SCC, neuron-specific enolase (NSE), and pro-gastrin-releasing peptide (Pro-GRP) better-distinguished lung cancer and lung disease, and lung cancer pathology types in Chinese patients [2]. In our previous study, we found that the 4MP significantly identified Chinese lung cancer patients from normal individuals [20]. The nodule risk model (4MP + nodule size) constructed by 4MP combined with nodule size has good potential in the benign-malignant differential diagnosis of lung nodules [20]. As our previous study was based on the results of a single-center study, we collected a new study cohort to validate the performance of 4MP in the differential diagnosis of benign nodule and early-stage lung cancer patients. In this research, our results showed that the AUC of 4MP in distinguishing early-stage lung cancer from Chinese benign lung nodule patients was 0.612 in the training cohort and 0.686 in the validation cohort. Therefore, we aim to improve the diagnostic performance of 4MP by combining the detection of other factors.
Clinical studies have demonstrated that benign or malignant lung nodules correlate with patients’ clinical characteristics and CT features of nodules. In the Mayo model incorporating patient age, history of cancer, cigarette-smoking status, spiculation, nodule diameter, and upper lobe location as predictors, the AUC value of the Mayo model was 0.833 [15]. However, researchers and clinicians have found that the Mayo model may not apply to Asians [40]. In the Brock model, age, gender, emphysema, family history of cancer, nodule size, total nodule number, solid nodule, spiculation parameters, and upper lobe involvement are used, and the Brock model with AUCs of at least 0.94 in an external validation cohort [41]. Previous research found that differences in disease prevalence and environmental factors may have led to the limited applicability of the Brock model in Asian populations, which had an AUC of 0.58 to 0.71 in the Chinese cohort [32]. In recent years, researchers have made several advances in the study of differential diagnosis and treatment of benign and malignant nodules. Miao et al. proposed a deep learning model combining CT images of lung nodules and intrathoracic fat images to differentiate between benign and malignant lung nodules, which significantly outperformed the model using CT images of lung nodules alone with an AUC of 0.910, 0.922, and 0.899 in the internal and external test cohorts, respectively [42]. Zhao et al. proposed the MAEMC-NET model based on self-supervised learning, which can effectively distinguish between benign and malignant isolated lung nodules by analyzing CT images of patients, and the AUC value of the model is 0.962 [43]. Meng et al. constructed a new risk stratification model cLung-RADS®v2022 based on Lung-RADS®v2022 and CT features for predicting invasive pure ground-glass nodules in China, which had an AUC value of 0.718 and 0.693 in the training and validation sets, respectively [44]. We analyzed the diagnostic effects of clinical characteristics (age, gender, BMI, drinking history, smoking history, family and personal history of cancer), CT features of nodules (size, number, margin, density, and shape) in Chinese benign nodules patients and early-stage lung cancer patients. We found that the AUC values for clinical characteristics and CT features of nodules were 0.628 and 0.726, respectively.
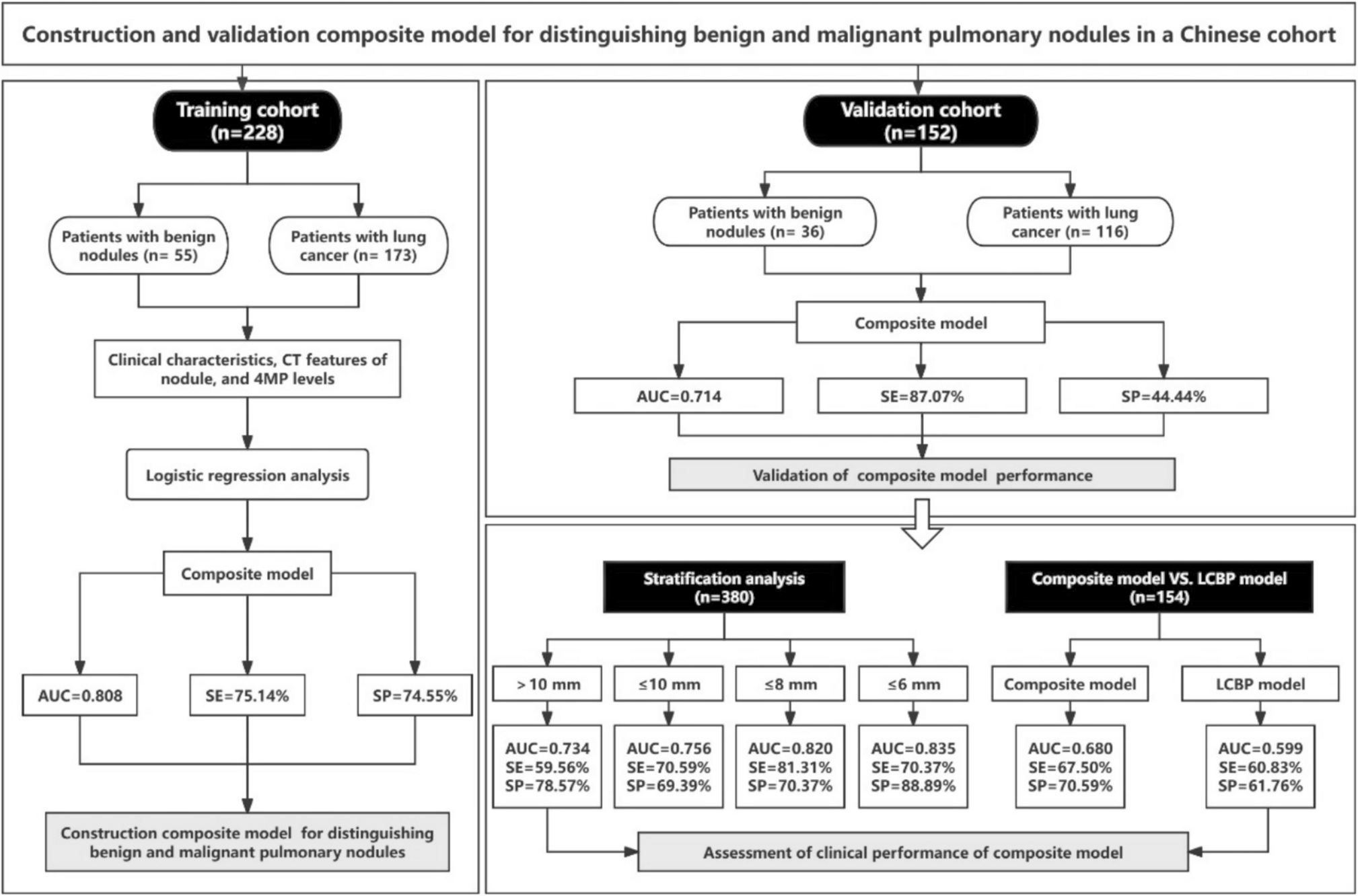
Related studies have shown that blood biomarkers combined with clinical characteristics can significantly improve the predictive performance of risk models for early malignant lung nodules. Xu et al. constructed a network diagnostic model consisting of seven autoantibodies (CAGE, PGP9.5, GAGE7, MAGEA1, SOX2, GUB4-5, and P53), clinical characteristics (age, cancer history, smoking history), and imaging features (nodules size, total nodule number, property of nodule, spiculation, lobulated sign, vessel sign, bubble-like sign, and pleural indentation) for the diagnosis of lung nodules, which had an AUC value of 0.96 [45]. In addition, Yang et al. developed the LCBP nodule risk model; in the training cohort, the AUC of the nodule risk model was 0.9151, but in the validation cohort, the AUC was only 0.5836 [17]. Hou et al. developed a predictive model based on CEA, CYFRA21-1, and CT features to differentiate between benign and malignant lung nodules, which achieved an AUC of 0.85 and 0.76 in the training and validation groups, respectively [18]. In this study, we screened out 7 factors of patient clinical information and CT features of nodule and developed a novel composite model that integrated 4MP, clinical characteristics (age, gender, BMI, family history of cancer), and CT features of nodule (nodule size, nodule margin, and nodule density). This study found that the novel composite model had a good predictive performance, with an AUC value of 0.808 in the training cohort and 0.714 in the validation cohort.
In lung cancer screening, based on primarily retrospective analyses of data from the International Early Lung Cancer Action Program and the NLST data, it is generally accepted that 6.0 mm is the threshold for positive results on the baseline scan [46]. It is important to note that this does not mean that cancers smaller than 6.0 mm cannot be detected on a baseline scan, it just means that they have a low incidence of malignancy [46]. The probability of malignancy is 1–2% for nodules 6–8 mm and less than 1% for all nodules smaller than 6 mm [12]. In the NLST, the lung cancer probability was 0.3% when the nodule diameter was 4–6 mm [47]. Texas MD Anderson Cancer Center studies have shown that in patients with nodule size ≤ 6 mm, the panel of nodule size + 4MP combinations performed exceptionally well, with an AUC of 0.95 [35]. Surprisingly, we found that the AUC values of the composite model were 0.820 and 0.835 in patients with ≤ 8 mm or ≤ 6 mm pulmonary nodules, respectively. Besides, the performance of the composite model (AUC = 0.680) was better than that of the LCBP nodule risk model (AUC = 0.599). These observations suggest that the new composite model has high performance in identifying benign lung nodules and early-stage lung cancer in Chinese patients and may show higher performance in smaller nodules. The new composite model is suitable for the adjunctive diagnosis of early-stage lung cancer patients, and when LDCT is used to screen people at high risk of lung cancer, patients with difficult-to-identify lung nodules can be further diagnosed by combining the patient’s clinical characteristics, biomarker levels, and CT features.
There are several limitations to this study. Firstly, although we analyzed the performance of the 4MP with patient data from different hospitals, continued multicentre studies are needed to comprehensively assess the applicability of the 4MP. Second, the new composite model relies on the characteristics of CT images, which may reduce the applicability of the model in certain resource-limited areas where patients may not have access to CT scans. Finally, there is a need to expand the sample size, especially for patients with lung nodules ≤ 6 mm, which will be the focus of our future studies.


Comments (0)