This systematic review and meta-analysis adhered to the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [16] and was registered in advance on the International Prospective Register of Systematic Reviews (PROSPERO) platform (No. CRD42024522464). Prior to registration, we established the foundational information, detailed research design, methodological choices tailored to the specific research design, and conducted an initial literature review. Subsequently, we refined the pertinent information in accordance with the registration guidelines of the PROSPERO website, ensuring both the comprehensiveness and precision of the data. The website offers recommendations for revisions, and we are required to implement the necessary adjustments based on this feedback.
Literature search
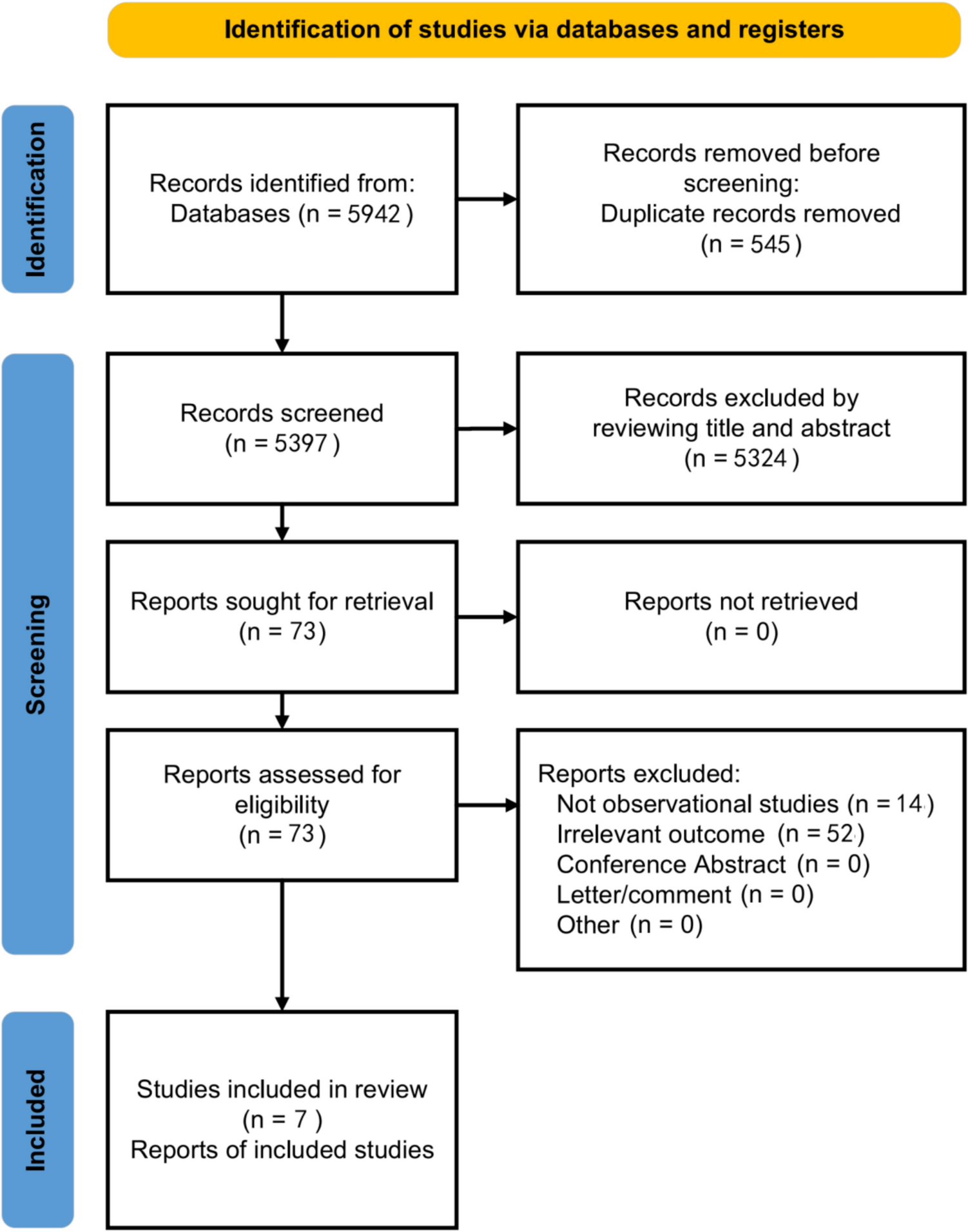
We conducted a comprehensive search of PubMed, Embase, and the Cochrane Library for relevant studies spanning from the inception of these databases to March 11th, 2024. Our search strategy utilized medical subject headings (MeSH) and synonyms for psoriasis and asthma, without any restrictions on geographical location or language. Details of the search strategy are provided in Supplementary Table 1.
Inclusion criteria and literature screening
The criteria for study selection included: (1) Observational studies that reported on the prevalence or risk factors of uveitis in psoriasis patients or vice versa, encompassing cohort, case–control, or cross-sectional designs. (2) For studies involving psoriasis patients as the case or exposure group, the control group consisted of individuals without psoriasis. Additionally, we excluded duplicate publications, conference abstracts, comments, letters, or studies with irrelevant findings. Studies utilizing the same cohort or having a sample size of less than 10 were also excluded. Study selection was performed independently by two authors (DDW and RC), who screened titles and abstracts and obtained full texts of potentially eligible studies. In cases of disagreement between the two authors, a third author (NL) resolved the discrepancy.
Data extraction
Data extraction was independently conducted by two authors (YP and JM) using a predefined form based on systematic review and meta-analysis guidelines [17]. Extracted baseline data encompassed first author, publication year, country, study design, participant demographics (age), duration of follow-up, diagnostic criteria used, sample size, adjustments made, and quality assessment. Disagreements were resolved through consensus discussion or by involving a third author (NL) for final adjudication.
Risk of bias assessment
Quality assessment of cohort and case–control studies was conducted using the Newcastle–Ottawa Scale (NOS) [18]. Scores ranging from 0 to 3, 4 to 6, and 7 to 9 indicated low, moderate, and high-quality studies, respectively. The assessment was independently performed by two authors (SRB and KLZ).
Statistical analysis
We utilized Stata 16.0 (Stata Corp, College Station, Texas) for data analysis investigating the association between psoriasis and uveitis. For case–control and cross-sectional studies, we computed odds ratios (ORs) with 95% confidence intervals (CIs), while for cohort studies, incidence rate ratios (IRRs) were calculated. Heterogeneity was assessed using I2 statistics. A fixed-effect model was employed if P > 0.1 and I2 ≤ 50%; otherwise, a random-effects model was used for I2 > 50%, indicating substantial heterogeneity. In cases of significant heterogeneity, sensitivity or subgroup analyses were conducted, with recalculations performed after excluding studies contributing to the heterogeneity. Funnel plots were generated to evaluate publication bias, and Begger’s and Egger’s tests were applied accordingly. Throughout the study, our primary focus was on assessing the influence of various factors on the meta-analysis outcomes. These factors encompass both demographic characteristics, such as age, gender, and race, as well as disease-related variables, including diagnostic criteria, disease severity, classification, and treatment modalities. We will strategically select relevant categories for more in-depth subgroup analysis, aiming to mitigate the impact of heterogeneity on our results.


Comments (0)