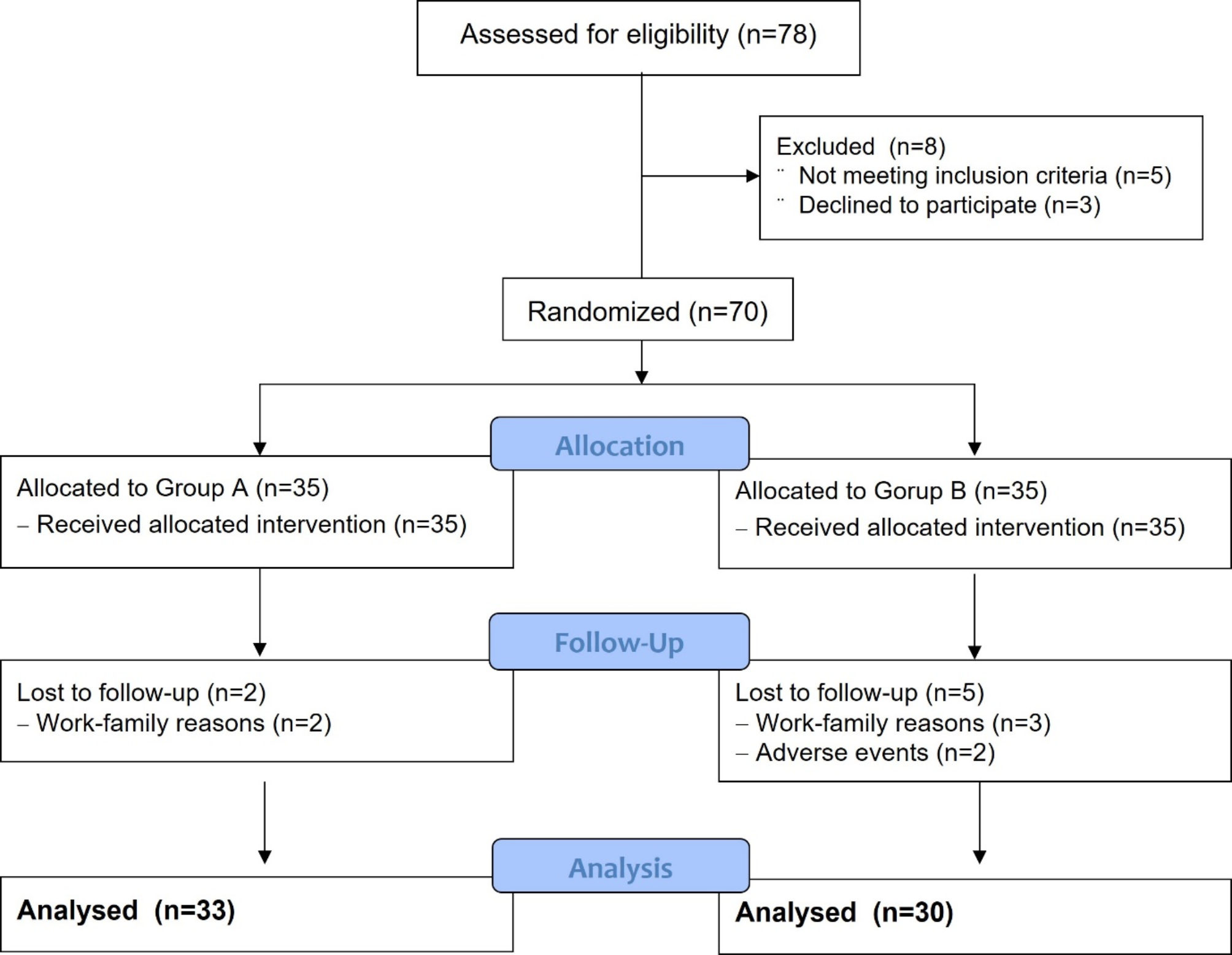
This study was a prospective, randomized, single-blinded multicenter trial conducted in three hospitals involving 70 patients aged 19–65 years. Approval was obtained from our institutional review board (IS19MIME0059), and the trial was registered with the Clinical Research Information Service (CRIS, KCT0007008). Written informed consent was obtained from all the participants.
Inclusion criteria included patients with rotatory ankle fractures (unimalleolar, bimalleolar, or trimalleolar fractures) who underwent operative fixation within two weeks of trauma under general anesthesia. Exclusion criteria included patients with pilon, open, or multiple fractures other than ankle fractures, those undergoing spinal anesthesia, those not opting for patient-controlled analgesia (PCA), individuals with Charcot arthropathy, chronic renal failure, diabetes mellitus for > 5 years, a history of angina pectoris or myocardial infarction within the last year, current use of pregabalin or NSAIDs, a previous surgical history of an ipsilateral ankle, ankle osteoarthritis, inflammatory arthritis, allergies to pregabalin or NSAIDs, and pregnant or nursing mothers.
According to an excel generated block randomization in the current study, the patients were stratified into two groups. Group A received naproxen 500 mg alone, and group B received naproxen 500 mg and pregabalin 75 mg, administered 2 h before surgery and then every 12 h for 14 days. Anesthesia was induced with propofol 1.5–2.5 mg/kg, rocuronium 0.6 mg/kg, remifentanil 0.2 mcg/kg/min, and sevoflurane 2–3 vol%. Anesthesia was maintained with sevoflurane and continuous remifentanil infusion (0.2 mcg/kg/min). During surgery, the following parameters were maintained: fraction of inspired oxygen (FiO2), 0.5; tidal volume, 6–8 mL/ideal body weight; and positive end expiratory pressure, 5 cmH2O. Respiratory rate was adjusted to maintain an end-tidal carbon dioxide of 35–40 mmHg. At the end of the surgery, muscle relaxation was reversed using neostigmine 1.5 mg and glycopyrrolate 0.4 mg. After airway device removal, the patient was transferred to a post-anesthetic care unit. The intravenous (IV) PCA regimen comprised citric acid fentanyl 8 µg/kg/day for those < 65 years old or 6 µg/kg/day for those > 65 years old, 100 mL of normal saline 0.9%, and ramosetron 0.3 mg. The infusion was programmed to be administered at 2 mL/h as a background infusion, with an additional 0.5 mL bolus available per demand, subject to a 15 min lockout period. Patient-controlled analgesia was initiated immediately after the operation was completed. In case of excessive pain, patients were given IV pethidine 25 mg as a rescue drug when their visual analog scale (VAS) score exceeded 5. Pethidine usage was permitted with a minimum of 4 h intervals and a maximum of six ampules per day, under the supervision of a physician. The time to first use and the quantity of ampules used were documented if used.
The VAS scores, along with any side effects, including indigestion, heartburn, general edema, dizziness, nausea, vomiting, and somnolence, were evaluated at 6, 12, 24, 48, and 72 h postoperatively. Patients were discharged three days after the operation, and prescribed the same medication to be taken in advance until 14 days postoperatively. Routine chemistry assessments, including aspartate aminotransferase, alanine aminotransferase, blood urea nitrogen, creatinine, radiographs, VAS scores, and the aforementioned side effects, were reviewed during the outpatient clinic visit at the two weeks mark. Subsequently, the patients were followed-up at three and six months postoperatively, with assessments, including VAS scores, Olerud and Molander score (OMS), and ankle-fracture outcome of rehabilitation measure (A-FORM). The use of A-FORM was permitted by the developer’s group, and both outcome measurements were validated tools for assessing recovery after ankle fractures [13]. A physician blinded to the current study evaluated all the outcomes.
Sample size calculation
We aimed to detect the minimally clinical important difference (MCID) between the groups in the VAS pain score at 1.8 of 10 [14]. A previous study showed that anticipated pain relief after use of those drugs were 3.55 (standard deviation [SD] = 1.36) and 2.57 (SD = 1.03), respectively [15]. We assumed a sample size of 35 patients in each group, with a 5% alpha set, 15% beta error, and 20% dropout rate using G power (version 3.1.9.4, Germany). The patients were divided into two groups based on block randomization generated in Excel, with a block size of 4.
Statistical analysis
An intention-to-treat analysis was employed, where the last data collected for patients who dropped out from further evaluations were used in subsequent analyses. Patient characteristics and clinical outcomes were presented as mean (SD) or count (percentage). The Shapiro–Wilk normality test was initially performed to assess the normal distribution of the study variables in the two groups. Upon confirmation of the normal distributions, the Student t-test for quantitative variables and chi-square test for categorical variables were used to compare between the groups. Pearson’s correlation test was used to evaluate correlations between fracture severity and other categories. Pearson’s rho values were interpreted as follows: little ( ± < 0.3), low (± 0.3–0.5), moderate (± 0.5–0.7), high (± 0.7–0.9), and very high ( ± > 0.9) [16]. Statistical significance was set at P < 0.05, and all statistical analyses were performed using Statistical Package for the Social Sciences (SPSS, version 25.0, IBM Corp., Armonk, NY, USA).





Comments (0)