
Remember me
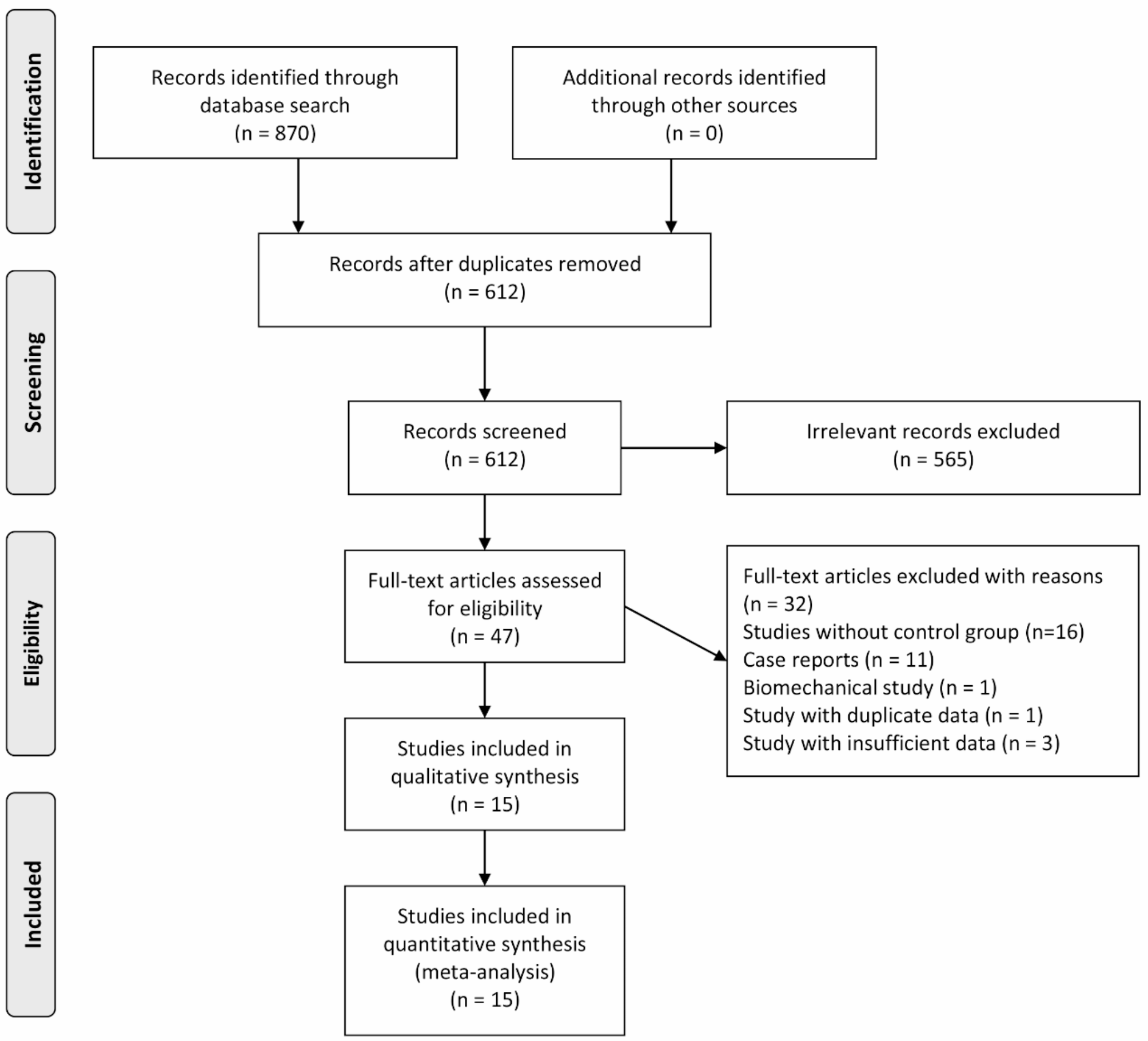




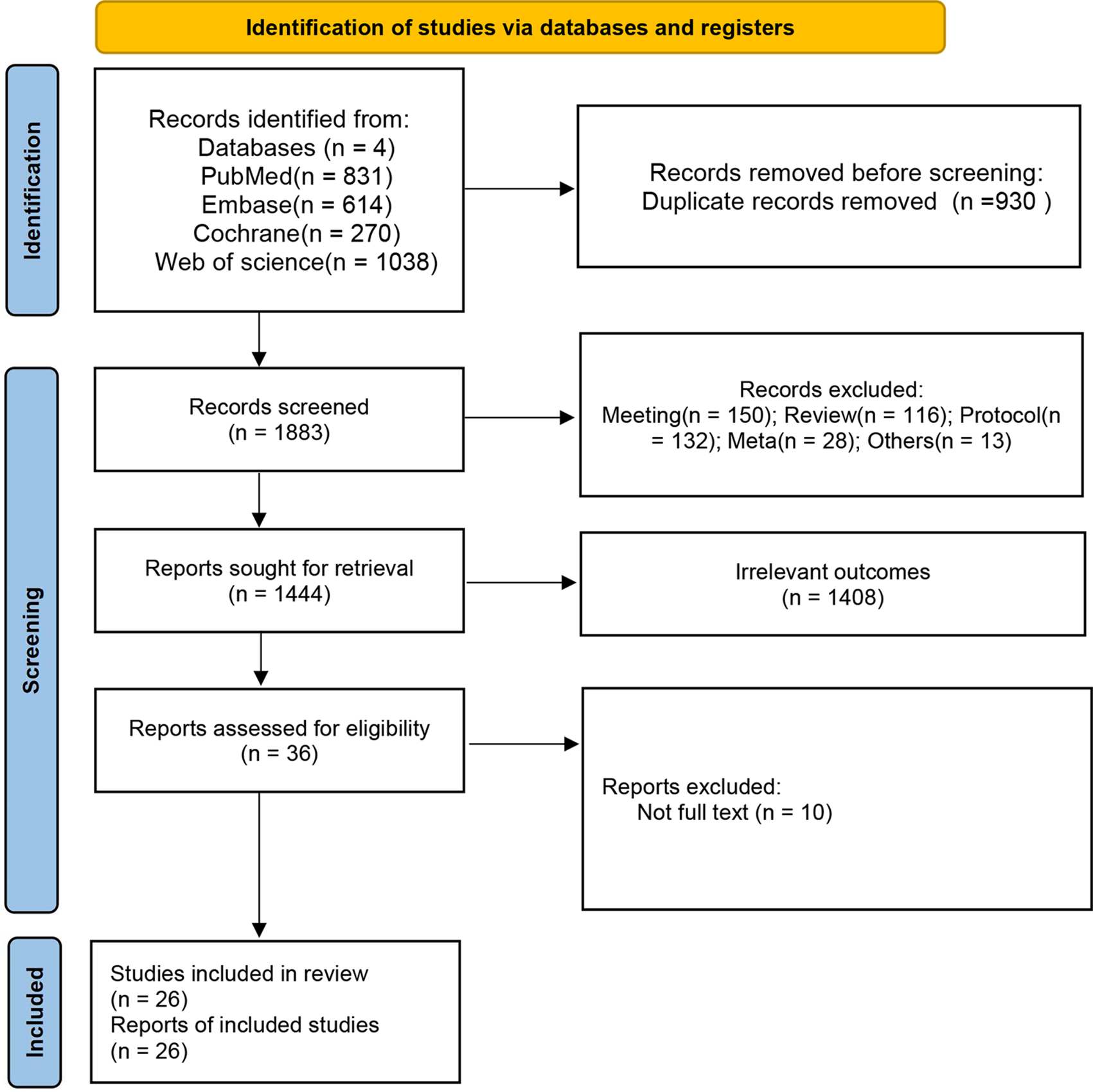
According to the pre-established literature retrieval strategy and collection method, a total of 2691 articles were obtained by computer retrieval, and 1783 related documents were obtained after eliminating 908 duplicates. According to the established criteria for inclusion and exclusion of articles, we read the titles and abstracts one by one on Endnote for document management, further excluded 1759 studies inconsistent with the inclusion criteria, and finally included 27 documents [28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54]. The flowchart is shown in Fig. 1.
Fig. 1
Flowchart of literature screening
Basic characteristics of the included studiesThere were 2579 patients in 27 studies, all over 30 years old. There was no statistical difference in baseline data between the two study groups in each study. The intervention measures included routine acupuncture, electroacupuncture, meridian-sinew theory-based treatment, warm needle acupuncture, fire needling, intensive silver needle therapy, electrical warm needling and auricular point application in the experimental group, and placebo needling, Western medicine (including diclofenac sodium, celebrex, loxoprofen sodium, acetaminophen and flurbiprofen gel for external use) and routine nursing in the control group. One of these articles is a three-arm experiment, the rest are two-arm experiments. One study is in a foreign language, and the rest are all in Chinese. In these studies, the outcome variables include VAS, ODI, RMDQ, JOA, overall response rate and recovery rate. The basic characteristics of the included articles are shown in Table 1.
Table 1 Basic characteristics of the included documentsDocument quality evaluation resultsAmong the 27 articles, 18 articles mentioned allocation by computer or random number table, and 2 articles involved allocation according to the order of treatment. There were 5 studies that used envelope for allocation concealment, 8 studies reported the blinding of participants and personnel, 21 reported the blinding of result evaluation, 9 RCTs reported the follow-up results of subjects, and 1 RCT did not show selective reporting. Except for these, other biases in all studies are unclear. The specific results for bias risk assessment are shown in Fig. 2.
Fig. 2 Inconsistency test
Inconsistency testP value was obtained by fitting inconsistency analysis. The overall response rate, recovery rate, ODI, JOA, RMDQ and VAS was 0.3902, 0.3642, 0.0643, 0.0527, 0.0825, and 0.0748, respectively. The above results show that the p-values were all greater than 0.05, which shows that the direct comparison and indirect comparison of various acupuncture treatments for CNLBP patients yielded consistent results. Node-splitting method was used to test local inconsistency, and the results showed that there was no statistical difference in overall response rate, ODI, JOA and RMDQ (P > 0.05), and there was no local inconsistency.
Network meta-analysis results of response rateOverall response rateNineteen RCTs [28, 29, 31,32,33, 35, 36, 38,39,40,41,42, 45, 48,49,50,51, 54] reported the overall response rate, involving six intervention methods: routine acupuncture, meridian-sinew theory-based treatment, electroacupuncture, auricular point application, warm needle acupuncture, fire needling, silver needle therapy and electrical warm needling, and control measures including placebo needling, routine nursing and Western medicine. The line connecting the dots of conventional acupuncture and meridian-sinew theory-based treatment was the thickest. There was a close loop formed by traditional acupuncture, meridian-sinew theory-based treatment, warm needle acupuncture, electroacupuncture, Western medicine and silver needle therapy. The overall response rate network diagram is shown in Additional file 2. The results of the league table show that the overall response rate of warm needle acupuncture, intensive silver needle therapy, meridian-sinew theory-based treatment, fire needling, electroacupuncture and routine acupuncture was higher than that of Western medicine. The overall response rate of intensive silver needle therapy, meridian-sinew theory-based treatment, fire needling, electroacupuncture and routine acupuncture was higher than that of placebo needling. The overall response rate of warm needle acupuncture, intensive silver needle therapy, meridian-sinew theory-based treatment, fire needling, electroacupuncture and routine acupuncture was higher than that of routine nursing. For the above comparisons, the P-values were less than 0.05, which is statistically significant. The detailed information on the overall response rate league table is shown in Table 2. The overall response rates of different intervention measures were ranked in descending order as follows: WAM (81.5), ISN (79.3), MMA (77.2), FN (66.0), EA (60.9), TA (45.1), WM (24.6), PN (10.9), and CC (4.6). The SUCRA diagram of the overall response rate is shown in Additional file 3.
Table 2 Overall response rate league tableRecovery rateEighteen RCTs [28, 31,32,33, 35, 36, 38,39,40,41,42, 44, 45, 48,49,50,51, 54] reporting the recovery rate were included for network analysis and involved 6 interventions (routine acupuncture, meridian-sinew theory-based treatment, electroacupuncture, auricular point application, warm needle acupuncture, fire needling, silver needle therapy and electrical warm needling) and control measures including placebo needling, routine nursing and Western medicine. The line connecting the dots of conventional acupuncture and meridian-sinew theory-based treatment was the thickest. There was a close loop formed by traditional acupuncture, meridian-sinew theory-based treatment, Western medicine, electroacupuncture, warm needle acupuncture, and silver needle therapy. The network diagram of the recovery rate is shown in Additional file 2. The results of the league table show that the recovery rate of warm needle acupuncture, fire needling, meridian-sinew theory-based treatment, intensive silver needle therapy and electroacupuncture was higher than that of Western medicine, and the recovery rate of fire needling, meridian-sinew theory-based treatment, intensive silver needle therapy, electroacupuncture and routine acupuncture was higher than that of routine nursing. For the above comparisons, the P-values were less than 0.05, which is statistically significant. The detailed league table of recovery rate is shown in Table 3. The SUCRA value of recovery rate for different intervention measures was ranked in descending order as follows: WAM (77.4), FN (76.3), MMA (70.3), ISN (61.4), EA (55.4), TA (34.8), WM (14.1), and CC (10.2). The SUCRA diagram of the recovery rate is shown in Additional file 3.
Table 3 Recovery rate league tableNetwork meta-analysis results of pain indicatorsVAS scoreTwenty-two RCTs [29, 31, 32, 35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50, 52,53,54] reported VAS, which involved 8 interventions, such as routine acupuncture, meridian-sinew theory-based treatment, electroacupuncture, auricular point application, warm needle acupuncture, fire needling, intensive silver needle therapy and electrical warm needling, and control measures including placebo needling, routine nursing and Western medicine. The connection between conventional acupuncture and meridian-sinew theory-based treatment, conventional acupuncture and electroacupuncture, and conventional acupuncture and placebo needling was the strongest. Traditional acupuncture, fire needling, Western medicine, meridian-sinew theory-based treatment and silver needle therapy, traditional acupuncture, fire needling, Western medicine and electroacupuncture form a closed loop. The network diagram of the VAS score is shown in Additional file 2. The results of the league table show that intensive silver needle therapy, warm needle acupuncture, meridian-sinew theory-based treatment, routine acupuncture, fire needling, auricular point application and electroacupuncture had better VAS scores than Western medicine. The VAS score of warm needle acupuncture, meridian-sinew theory-based treatment, fire needling, auricular point application and electroacupuncture was better than that of routine nursing. The VAS score of intensive silver needle therapy, warm needle acupuncture, meridian-sinew theory-based treatment, fire needling and electroacupuncture was better than that of the placebo needling. For the above comparisons, the P-values were less than 0.05 (Table 4). The detailed VAS score league table is shown in Table 4. The SUCRA value of VAS scores for different interventions in descending order were EN (92.8), ISN (78.6), WAM (62.8), MMA (59.4), TA (54.4), FN (53.5), AA (47.7), EA (42.4), WM (32.1), CC (16.8), and PN (9.5). The SUCRA diagram of the VAS score is shown in Additional file 3. The analysis of the VAS score difference obtained similar results, as shown in Table 4 and Additional files 3 and 4.
Table 4 VAS score league tableJOA scoresIn this network analysis, 10 RCTs [38, 39, 41, 44, 49,50,51,52,53,54] reported JOA score, which included seven intervention methods: routine acupuncture, meridian-sinew theory-based treatment, electroacupuncture, auricular point application, warm needle acupuncture, fire needling, intensive silver needle therapy and electrical warm needling, and three control measures: placebo needling, routine nursing and Western medicine. The connection between conventional acupuncture and electroacupuncture, conventional acupuncture and routine nursing, and conventional acupuncture and Western medicine was the strongest. Traditional acupuncture, Western medicine, meridian-sinew theory-based treatment, warming needle acupuncture, electroacupuncture and electrical warm needling form a closed loop. The network diagram of the JOA score is shown in Additional file 2. The results of the league table show that the JOA score of warm needle acupuncture, intensive silver needle therapy, routine acupuncture, electroacupuncture, meridian-sinew theory-based treatment and auricular point application was higher than that of Western medicine. While for warm needle acupuncture, electroacupuncture and meridian-sinew theory-based treatment, the JOA score was higher than that of routine nursing. For the above comparisons, the P-values were less than 0.05, which is statistically significant. The detailed JOA score league table is shown in Table 5. The SUCRA value of JOA score for different interventions in descending order was EN (99.7), WAM (72.4), ISN (64.6), TA (57.7), EA (56.6), MMA (41.1), AA (33.0), WM (21.2), and CC (3.8) (Additional file 3). The analysis of the JOA score difference obtained similar results, as shown in Table 5 and Additional files 3 and 4.
Table 5 JOA score league tableNetwork meta-analysis results of functional indicatorsODI scoresA total of 16 articles [28, 31, 32, 34, 36, 37, 39,40,41,42, 44, 46, 48, 49, 51, 54] reported ODI score and included five intervention methods, such as routine acupuncture, meridian-sinew theory-based treatment, electroacupuncture, fire needling and intensive silver needle therapy, and control measures, such as placebo needling, routine nursing and Western medicine. The connection between conventional acupuncture and meridian-sinew theory-based treatment was the strongest, which signifies multiple direct comparative studies. Among them, traditional acupuncture, meridian-sinew theory-based treatment, Western medicine and fire needling form a closed loop. The network diagram of the ODI score is shown in Additional file 2. The results of the league table show that the ODI score of meridian-sinew theory-based treatment,
Comments (0)