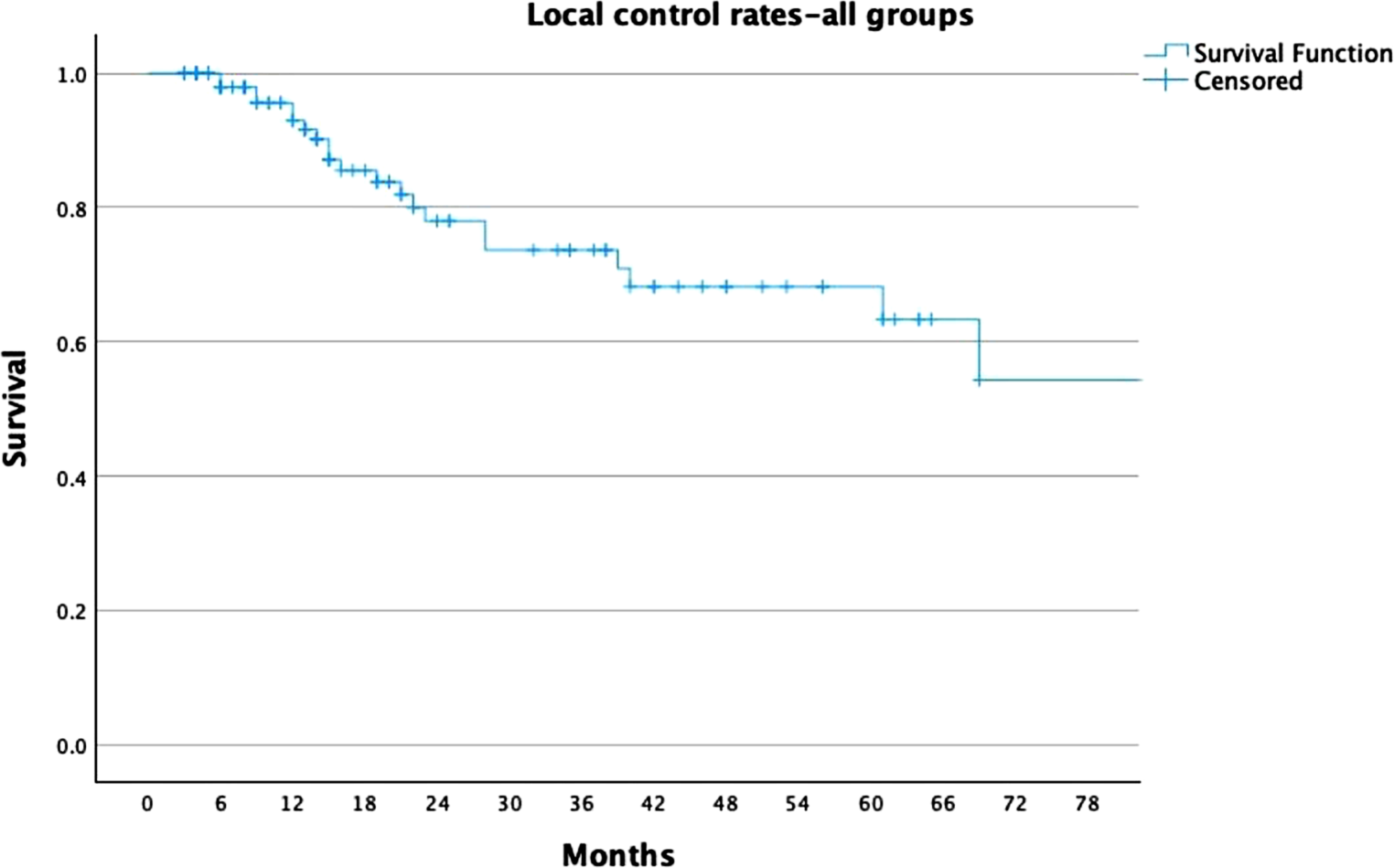
This study highlights the efficacy and safety of single-fraction SBRT (SF-SBRT) for primary NSCLC, with a specific focus on doses ≥ 30 Gy. Our findings demonstrate robust long-term LC and PFS, along with minimal toxicity, underscoring SF-SBRT as a viable alternative to multi-fraction protocols for select patient populations. The LC rates of 81% and 77% at 3, and 5 years for patients treated with ≥ 30 Gy affirm the dose-dependent effectiveness of SF-SBRT. These outcomes are consistent with those reported in previous studies, such as RTOG 0915 and others, which documented similar efficacy in dose-escalation trials [12, 13]. By contrast, patients receiving doses < 30 Gy exhibited significantly lower LC rates (53%, and 44% at 3, and 5 years), emphasizing the importance of dose optimization for achieving optimal tumor control. The PFS and OS analyses further support the superiority of higher doses. At 5 years, patients treated with ≥ 30 Gy achieved a PFS of 43%, compared to 17% in the < 30 Gy cohort. These findings corroborate previous research indicating that biologically effective dose (BED) thresholds, such as BED10 ≥ 100 Gy, play a crucial role in enhancing both local and systemic outcomes.
Our findings align closely with those of Singh et al., who reported comparable PFS, and OS rates between single-fraction and multi-fraction SBRT regimens for early-stage NSCLC [13]. Specifically, our 2‑year PFS of 68% for ≥ 30 Gy aligns with Singh’s 65% for a single 30 Gy fraction. However, our 2‑year OS of 84% exceeds their reported 73%, potentially reflecting differences in patient selection or comorbidities. Notably, our study demonstrated lower toxicity, with only 2% acute pneumonitis and no grade ≥ 3 events, compared to 16% thoracic grade 3 adverse events in Singh’s single-fraction cohort. These results reaffirm the efficacy and safety of high-dose single-fraction SBRT and highlight its advantages in reducing treatment burden while maintaining excellent clinical outcomes.
Our results are inferior with those of the RTOG 0915 trial, which compared single-fraction SBRT (34 Gy) to multi-fraction SBRT (48 Gy in 4 fractions) in patients with peripheral NSCLC. Both studies demonstrated high long-term local control rates, with RTOG reporting 5‑year primary tumor failure rates of 10.6% and 6.8% for single- and multi-fraction arms, respectively, comparable to the 77% 5‑year local control achieved in our high-dose single-fraction cohort. PFS and OS also align, with RTOG showing median OS of 4.1–4.6 years and 5‑year OS of 29.6%–41.1%, similar to the 5‑year OS of 63% observed in our high-dose group. Importantly, both studies confirmed the low toxicity profile of single-fraction SBRT, with RTOG reporting 2.6% grade 3 toxicity, comparable to our finding of no grade 3 or higher events. These findings collectively reinforce the efficacy and safety of single-fraction SBRT for early-stage, inoperable NSCLC, offering excellent clinical outcomes with reduced treatment burden.
Stanford University released the initial prospective studies on dose-escalation in 2003. The authors subsequently reported the results at a variety of concentrations [14, 15]. The research design of this Phase I trial was centered on dosage escalation, with four doses of single-fraction ranging from 15 Gy to 30 Gy, gradually increasing by 5 Gy.
The primary goal was to determine the maximum tolerated dose (MTD) of SF three months after administration. There was a total of 32 inoperable patients, 20 of whom had NSCLC and 12 of whom had metastatic lesions that were less than 5 cm in size. Individuals with central tumors and a PTV greater than 50 cc exhibited Grade 2–3 pneumonitis after 5–6 months. In contrast, the administration of 25 Gy to patients who had a history of radiation led to a significant increase in the severity of the adverse effects. In order to exclude individuals with a PTV greater than 50 cc who had previously undergone radiation therapy, an additional modification was made to the 30 Gy dose. The three G5 toxicities that were recorded were linked to centrally located tumors in patients who had previously undergone chemotherapy. One patient received treatment prior to SABR, while the other two received it as adjuvant therapy to SBRT. Additionally, two of the patients had a PTV exceeding 50 cc. At one year, the LC rate was 91% for patients who received a dose exceeding 20 Gy and 54% for those who received a dose below 20 Gy. Metastatic lesions exhibited significantly inferior LC in comparison to basic tumors. The authors have determined that SF SBRT at a dosage of 25 Gy is well-tolerated in patients with a history of thoracic radiotherapy and a PTV of less than 50 cc. However, the cohort that has undergone prior chemotherapy, either prior to or following SBRT, and central lesions may be at an increased risk.
Additionally, this study is the first to assess the Charlson Comorbidity Index (CCI) as a predictor of OS. The Cox proportional hazards analysis identified the Kaplan-Meier method as the sole factor to exhibit a statistically significant trend, demonstrating improved OS for patients with CCI scores less than 8. This suggests that the primary determinant of OS in this relatively frail patient cohort is overall health status. Furthermore, it underscores the utility of the CCI in this context.
A German study has similarly focused on evaluating prognosis in patients with early-stage lung cancer using the Age-adjusted Charlson Comorbidity Index (aCCI) [16]. Dreyer et al. analyzed baseline comorbidities and their impact on clinical outcomes in a cohort of 196 patients. The median OS was 15.0 months, attributed to advanced age and competing comorbidities. The aCCI was used to assess prognosis, revealing that patients with an aCCI of 8 or higher had significantly higher risks of death and cancer-specific mortality than those with an aCCI of 7 or lower. Compared to the Cumulative Illness Rating Scale for Geriatrics (CIRS-G), the aCCI is quicker and more accessible for clinical application. Although the CIRS‑G has not been widely used in large cohorts of medically inoperable lung cancer patients treated with SBRT, the aCCI effectively assessed survival outcomes in this population. It was demonstrated to be a reliable prognostic tool. Furthermore, Dreyer et al. reported that the clinically relevant radiation pneumonitis ≥ 2 rate was 12.7% in this primarily multimorbid patient collective, which was not abnormally elevated. In this context, Kowalchuk et al. identified three tumor-specific factors that warrant further investigation for their potential influence on OS: BED, tumor size, and pre-treatment SUV [17]. Their research revealed a Kaplan-Meier analysis trend and an OS benefit with increased BED (≥ 120 Gy) in univariate analysis. Interestingly, this threshold is higher than that of earlier studies, which observed improved LC with BED10 ≥ 100 Gy [18]. However, in our study, treatments with BED10 ≥ 100 Gy did not demonstrate a corresponding improvement in OS.
These findings align with those of Pennathur et al. [19], who conducted a retrospective study on 100 patients treated with SBRT for recurrent tumors using various regimens, including single-fraction SBRT and multi-fraction schedules (45–60 Gy in 3–5 fractions). They reported 5‑year OS rates of approximately 57%, with 1‑, 2‑, and 5‑year OS rates of 74%, 49%, and 31%, respectively, and a median follow-up of 51 months. This study demonstrated promising outcomes for SBRT in oligo-recurrent or oligo-progressive lung cancer, with no significant adverse effects.
In our cohort, multivariate analysis indicated that comorbidities and age significantly influenced OS, highlighting the importance of patient selection to achieve optimal long-term outcomes. Our study’s safety profile is also noteworthy, with no grade 3 or higher toxicities and a late pneumonitis rate of 21%.
These findings are consistent with those of Tekatli et al. [20], who reported similarly low toxicity rates (≤ 2%) for single-fraction SBRT in patients with synchronous lung malignancies. In their retrospective analysis of 84 patients with 188 pulmonary lesions treated for primary and metastatic synchronous tumors, only seven lesions (3.7%) were treated with a single 34 Gy fraction using multicentric VMAT for spatially separated lesions. Grade 3 or higher toxicities were observed in just 2% of patients. In our study, even with high-dose regimens, safety was evident, with acute pneumonitis occurring in only two cases.
Additionally, Kumar et al. [21] compiled data on 445 patients with early-stage NSCLC treated with SBRT at the Cleveland Clinic. This cohort included 26 patients (5.8%) with synchronous lung tumors confirmed by biopsy and/or PET-CT. All patients, whether treated for synchronous or solitary tumors, received single-fraction SBRT at doses of 30 Gy or 34 Gy. After one year, no significant differences in progression or survival rates were observed between the two groups.
Single-fraction SBRT is also economically advantageous. In light of rising healthcare costs, cost-effective and efficient RT options should be prioritized. This is particularly relevant in the United States, where the Centers for Medicare and Medicaid Services are transitioning from fee-for-service to episode-based payment models to improve cost efficiency [22]. SF SBRT offers substantial financial savings, as its costs are estimated to be 40% lower than those of three-fraction regimens, based on 2009 Medicare prices [23]. During the COVID-19 pandemic, single-fraction regimens can further reduce costs by minimizing the use of personal protective equipment and clinical resources. This study acknowledges its limitations, including its retrospective design, single-institution scope, and lack of comprehensive toxicity data. Additionally, certain NSCLC subtypes, such as lepidic pattern adenocarcinoma, which is characterized by its indolent behavior and lower metastatic potential, were excluded [24, 25]. However, our findings indicate that toxicity associated with single-fraction SBRT, even in chest wall cases, remains low. Future prospective, multicenter trials are needed to validate these results, refine patient selection criteria, and explore biomarkers for treatment response.
While our findings indicate favorable long-term outcomes and a strong safety profile for high-dose single-fraction SBRT in NSCLC, several limitations must be acknowledged. Most importantly, the reliability of LC, PFS, and OS outcomes is highest in patients with histologically confirmed NSCLC. In patients without biopsy confirmation, even FDG-PET-positive lesions may represent benign conditions such as inflammation or infection, which can radiologically mimic malignancy. Consequently, the inclusion of PET-positive but histologically unverified lesions introduces the risk of misclassifying benign nodules as malignant, potentially leading to an overestimation of LC and PFS following SBRT. To account for this limitation, we conducted separate analyses for the entire cohort and for the subset of patients with histologically confirmed diagnoses. Future prospective studies should prioritize histopathologic confirmation to ensure the validity and accuracy of survival outcomes and treatment efficacy assessments.
Table 4 provides a literature review of studies involving non-small-cell lung cancer patients treated with stereotactic radiotherapy.
Table 4 Literature review for non-small-cell lung cancer patients treated with stereotactic radiotherapy


Comments (0)