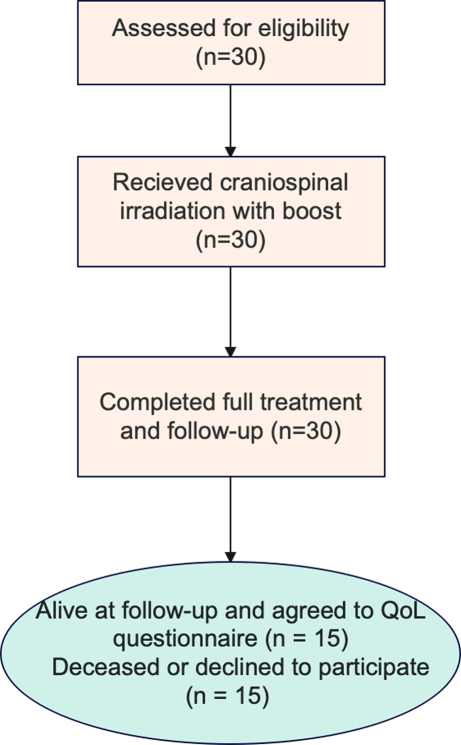
This is a retrospective, single-center study including locally Advanced Cervical Cancer (LACC) patients (Fédération Internationale de Gynécologie et dʼObstétrique [FIGO] 2018 stage from IB3 to IVA), treated at Policlinico Agostino Gemelli IRCCS with exclusive radiochemotherapy between January and December 2020 and followed for almost 5 years.
During the follow-up, the patients underwent gynecological clinical visits with pap test and radiological exams, if necessary.
In particular, pelvic MRI scan performed according to the following timeline: baseline, prior brachytherapy, 3 and 6 months after the end of overall treatment. Patients younger than 18 years, without pretreatment MRI, treated with palliative intent or those who did not undergo biopsy for histological confirmation of response, were excluded from the analysis. Table 1 summarizes a complete description of the cohorts investigated in this study.
Table 1 Patient characteristicsTreatments
All patients underwent definitive radiochemotherapy. Radiotherapy volumes were delineated according to consensus guidelines [22].
Concurrent chemotherapy was administrated with cisplatin alone. Radiotherapy was delivered to the primary tumor, cervix, parametria, uterus, vagina until 3 cm below the inferior margin of the tumor and regional nodes (common, presacral, internal, external iliacs and obturators) for a total dose of 45 Gy in 25 fractions over 5 weeks. Involved lymph nodes were boosted using simultaneous integrated boost (SIB) with a dose of 55 Gy in 25 fractions for pelvic lymph nodes, and 57.5 Gy in 25 fractions for aortic lymph nodes.
Volumetric modulated arc therapy technique was used with daily image guidance and couch correction according to bony structures or planning target volume (PTV).
High-dose rate intracavitary/interstitial brachytherapy (HDR-BT) with an iridium source and Fletcher or Venezia applicators was performed within a week of the completion of external beam radiotherapy. The combination of interstitial and intracavitary brachytherapy was used for tumors with parametrial invasion or lateral pelvic wall involvement. Combined intracavitary/interstitial brachytherapy was performed in 30% of patients, while the remaining 70% received intracavitary brachytherapy alone.
It was delivered twice a week for 2 weeks in a row using the microselectron digital brachytherapy afterloader. A planning computed tomography (CT) scan was obtained before the delivery of fractions 1 and 3. The high-risk clinical target volume (HR-CTV) and organs at risk were contoured on the planning CT according to the GEC-ESTRO guidelines [16] after fusion with T2-weighted MRI images.
The residual gross tumor volume (GTV; compared to initial GTV) and the “gray zones” observed in the parametria on T2, were used to define the HR-CTV. A total dose of 28 Gy in 4 fractions to HR-CTV and 14 Gy in 2 fractions to IR-CTV was administered. The dose to > 2 cc of the sigmoid colon, rectal and bladder volume was limited to EQD2 < 75 Gy, < 75 Gy and < 90 Gy, respectively.
Response assessment/treatment outcome
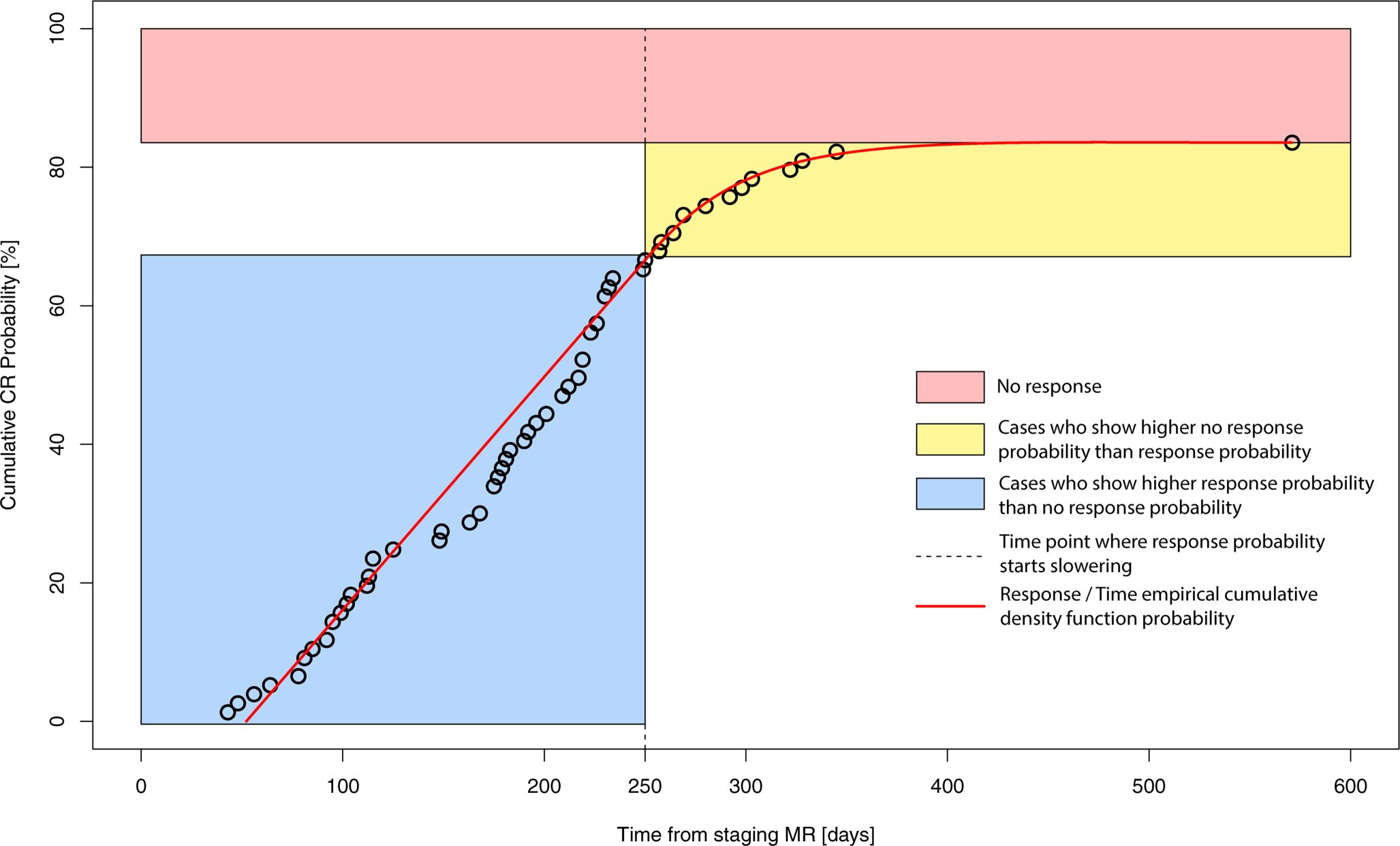
The primary endpoint was the radiological complete response (CR) evaluation, analyzed at three timepoints with MRI:
First assessment: before IRT, at the end of external beam irradiation (5–6 weeks from the start of treatment),
Second assessment: 3 months following the completion of the IRT (18–20 weeks from the start of treatment), and
Third assessment: 6 months after the IRT has ended (30–32 weeks from the start of treatment).
Response was assessed according to Response Evaluation Criteria in Solid Tumors from dedicated radiologists [23].
According to radiological response at each assessment, patients were divided into four groups: radiological complete response (cCR), defined as absence of disease at MRI imaging; radiological partial response (cPR), defined as a decrease of at least 30% from baseline in the sum of the diameters of the target lesions; stable disease (cSD) defined as any cases that do not qualify for cCR, cPR or disease progression (cPD), confirmed by biopsy. Patients who attended exams but provided insufficient response data were labeled “unknown,” whereas those who did not attend assessments or did not provide data were labeled “missing.”
During the analysis, patients were divided into two groups, those who achieved cCR and those who did not, with the non-cCR group including patients with cPR, cSD and cPD.
Patients were scanned with a 1.5 T MR scanner (Echospeed Horizon and Infinity, General Electric Healthcare, Chicago, IL, USA) using a standard 8‑channel phased-array body coil without contrast.
Technical parameters are reported in the Supplementary Table.
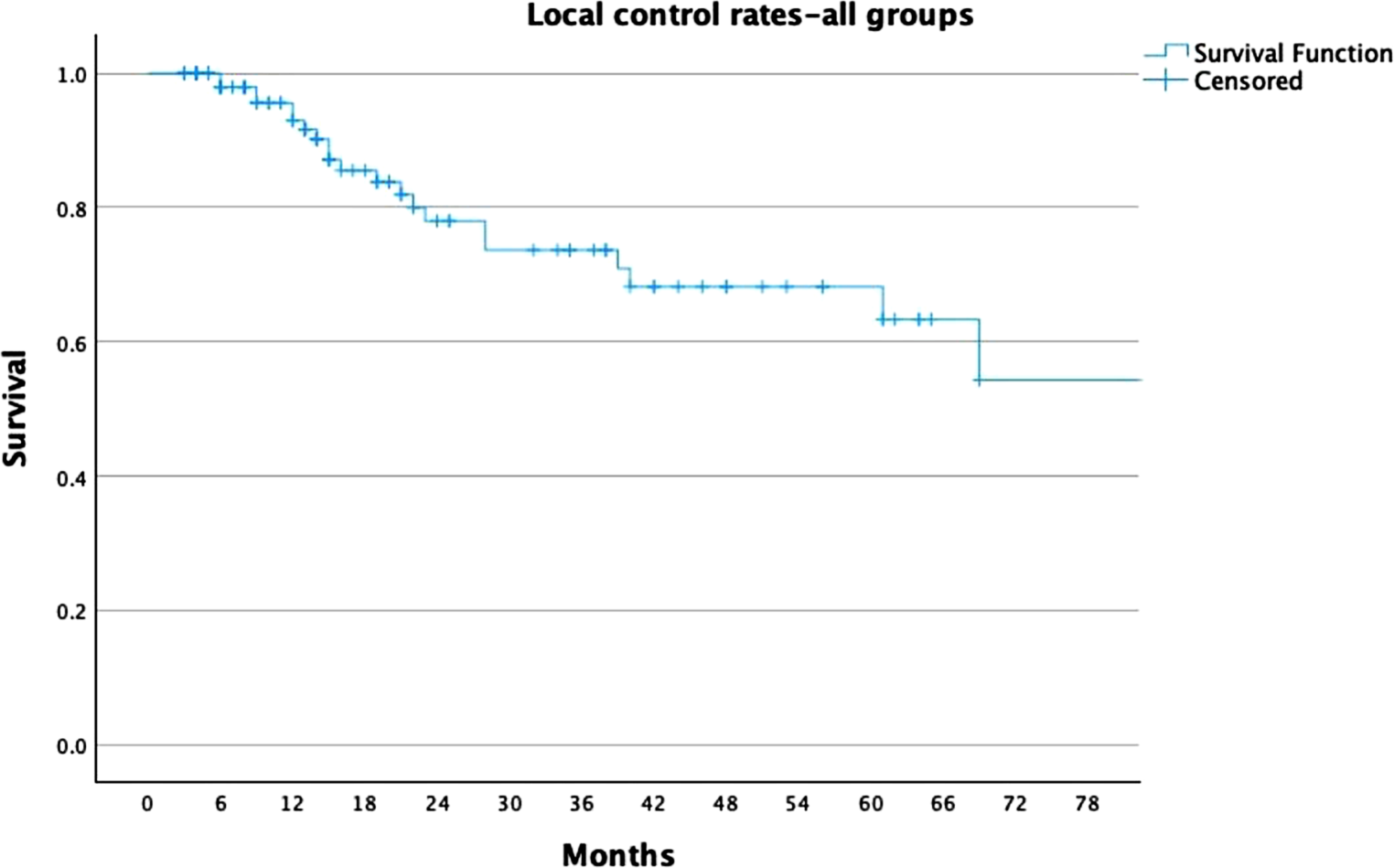
Overall survival and disease-free survival for the overall trial population and the subgroup of patients with a complete response at all timepoints were analyzed.
Statistical analysis
Continues variables were expressed as mean and standard deviation and compared using unpaired two-sample Student’s t‑tests, whereas categorical variables were expressed as numbers and percentages and compared using χ2 tests. Variables possibly associated with CR (stage, histology, age, grading) were evaluated by logistic regression analysis, with the resulting predictive model validated by receiver operating characteristics curve analysis (ROC).
Disease-free survival (DFS) was calculated from the date of diagnosis to the date of relapse or the date of the last follow-up; overall survival (OS) was calculated from the date of diagnosis to the date of death or the date of the last follow-up. Survival curves were presented as Kaplan–Meier plots [24]. Statistical Package for Social Sciences software version 25.0 (IBM Corporation, Armonk, NY, USA) and Stata software version 13.0 (StataCorp, College Station, TX, USA) were used for statistical analysis.
All p values were two-sided, and a p value < 0.05 was considered statistically significant.


Comments (0)