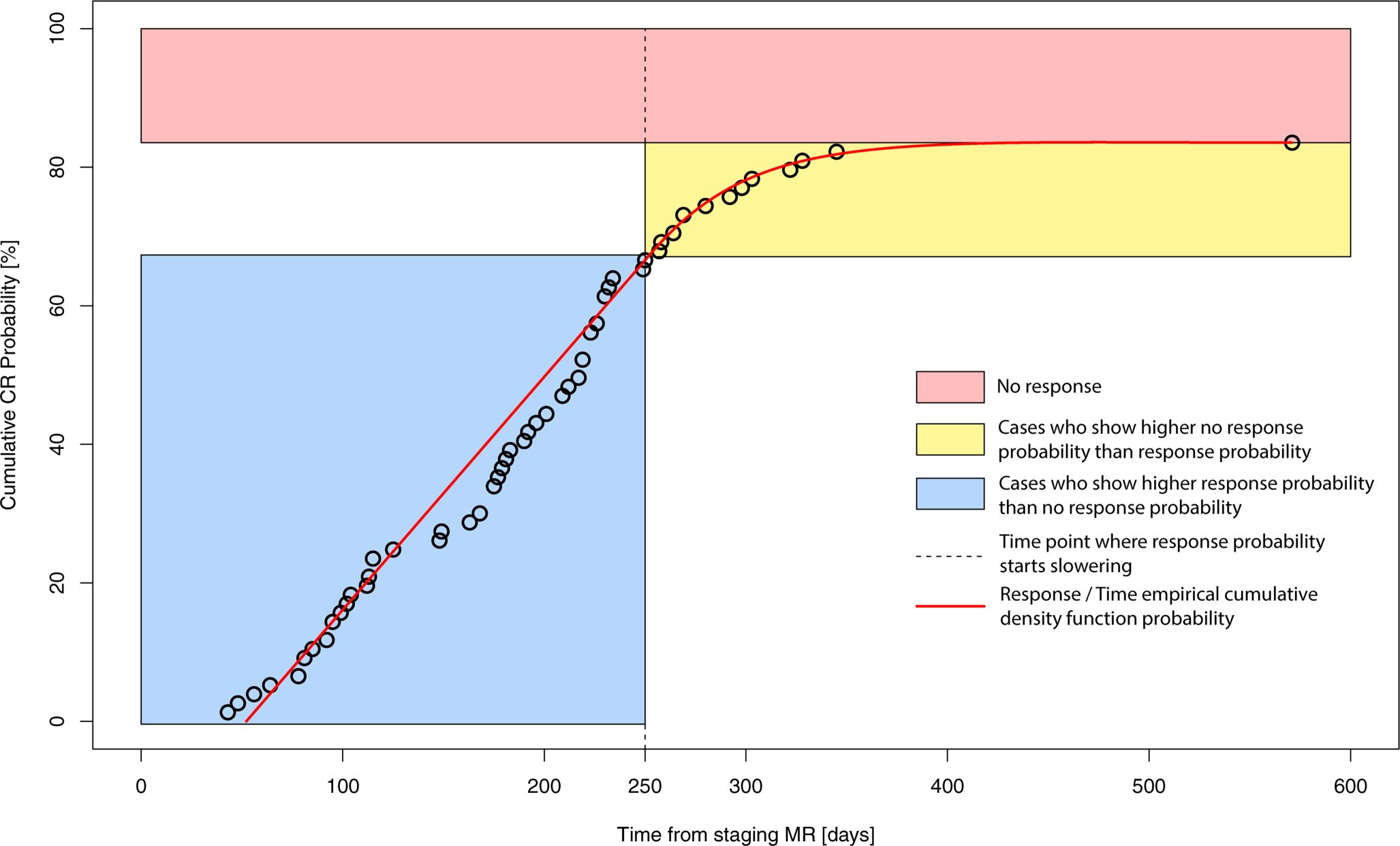
This ultra-hypofractionated irradiation schedule using five consecutive fractions for locally advanced breast cancer is well tolerated. In addition, a good clinical response was observed in almost all studied inoperable and/or frail patients. Adverse effects were rare, and almost all patients showed a good clinical response within the first 90 days after completion of local therapy.
While there is a need to develop hypofractionated radiotherapy concepts in a patient population with advanced tumor disease, the optimal regimen remains unclear [26]. The previous literature presents other experiences of hypofractionated palliative radiotherapy in locally advanced cancer and fungating wounds [29]. For example, palliative hemostatic radiotherapy was proven to be effective in the treatment of advanced pelvic gynecological malignancies. Meixner et al. investigated different fractionation schemes and observed a biologically effective dose (BED) cut-off value of BEDα/β = 10 = 36 Gy [25]. They reported high cessation of bleeding (80%) and good pain relief (60%) in their cohort. Furthermore, in non-melanoma skin cancer, hypofractionated radiation therapy was established to be effective and well tolerated, with a wide range in BEDα/β = 10 from 30 to over 157 Gy [28]. In addition, it has been found that in the treatment of pelvic malignancies of different tumor entities with gross hematuria, a BEDα/β = 10 ≥ 36 Gy is required for symptom relief [27]. In our fractionation scheme, we apply a BEDα/β = 10 = 37.5 Gy, and to offer relief to the surrounding organs at risk, we apply a BEDα/β = 10 = 45 Gy as a simultaneous integrated boost to the primary gross tumor volume.
Various hypofractionated radiation regimens have already been published for this patient population. An overview of studies with similar palliative radiotherapy concepts is shown in Table 5.
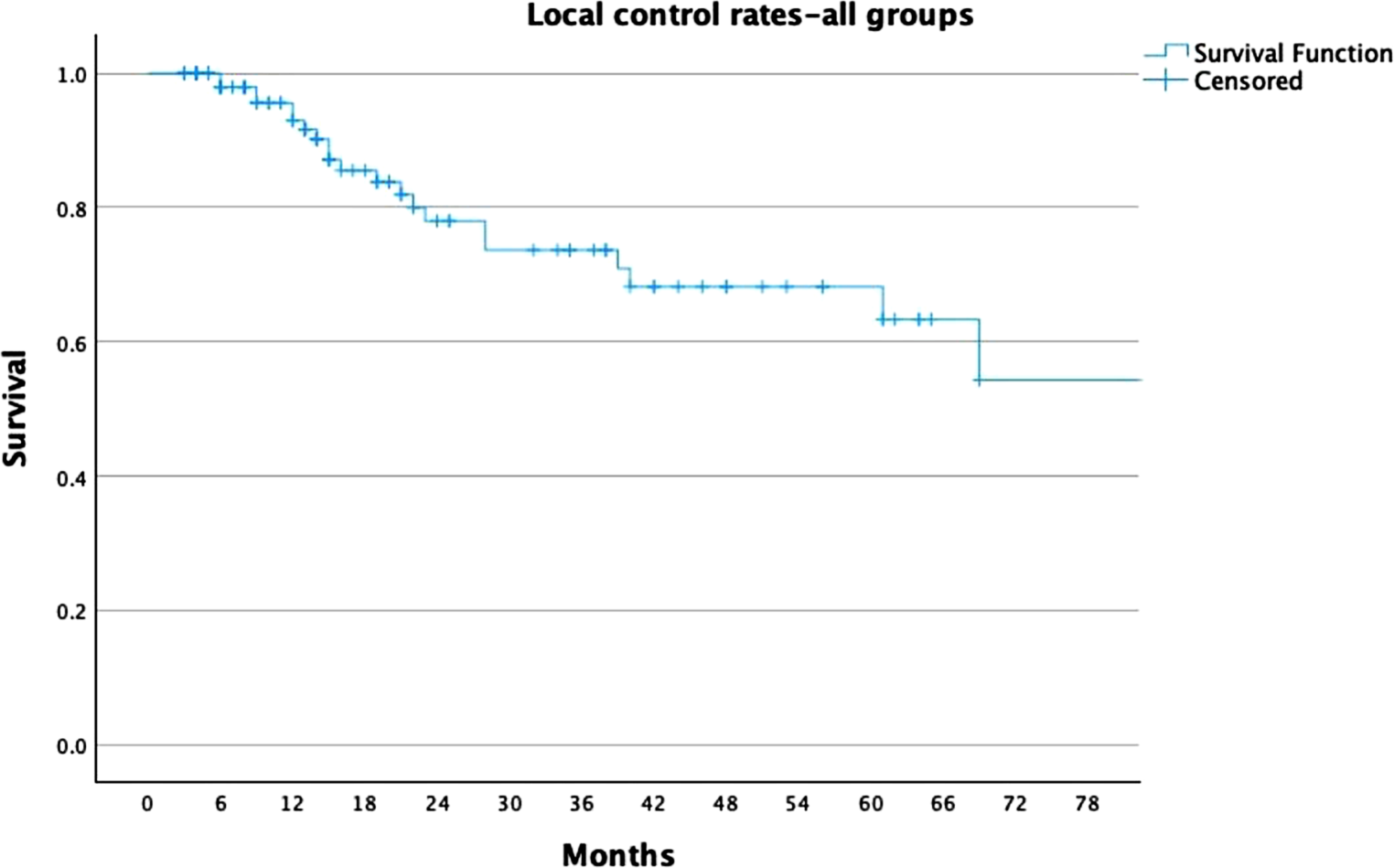
Table 5 Overview of studies with similar palliative radiotherapy conceptsThe radiation concept shown in our study is completed within a very short overall treatment time (maximum treatment period of up to 2 weeks). The tolerability is excellent, with maximally grade 1 toxicity locally in the radiation field and no higher-grade toxicities, unlike other studies that have described grade 2 skin toxicity. Our data also show excellent local control rates compared to the other studies, with very little local progression after local radiation therapy (only 3% of patients showed local progression and no improvement in symptom burden).
In the palliative setting, it is important to shorten the overall treatment time for patients, to reduce transport times and hospital stays. Giving irradiation treatment twice to three times per week allows time for normal tissue to recover before repopulation of tumor cells, as shown in palliative treatment in other tumor entities [23].
As shown in Table 5, several schemes for fractionation have already been established in the field of palliative radiotherapy for advanced breast cancer. Choi et al. [16] established a radiation concept with total doses of up 42.5–55 Gy with 2.5–3 Gy per fraction once per day, 5 days a week. In this cohort, the authors noted good symptom relief and a strong response in terms of local tumor control (over 80% partial response or stable disease). Nevertheless, over 70% of the treated patients experienced grade 2 moist desquamation of the skin, which is a greater percentage than reported in our study. The overall treatment time in this cohort was 3–5.5 weeks. With our fractionation concept, patients are finished with radiotherapy in 2–3 weeks, which saves time and avoids delaying any systemic therapies that may be indicated. Hoeltgen et al. [20] analyzed different concepts with a wide range of doses: median BED 68.3 Gy (range 40.0–94.5) and EQD2 45.5 Gy (range 26.7–63.0). The cumulative RT dose most frequently used in this work was either 39 or 45 Gy with a single dose of 3 Gy. Symptom palliation was reported in 95% of patients with low-grade side effects, predominantly erythema and fatigue. This study describes effective concepts that can be further shortened with even stronger hypofractionation, as in our concept, with similar effectiveness and tolerability.
Similar to our fractionation concept, in other studies, patients were irradiated with single doses of 6 Gy (Webb et al. [22]) or 6.5 Gy (Courdi et al. [19]) in somewhat larger cohorts. Webb et al. [22] compared once-weekly versus accelerated fractionation schedules in their cohort with 6‑Gy fractions over 6 weeks, administering up to 30 Gy to the whole breast and involved lymph nodes with or without a 6-Gy boost to the affected tumor quadrant (total dose not exceeding 36 Gy). They reported no significant difference in the groups regarding the median time to local progression or toxicity, but one patient who received five fractions a week suffered from grade 4 late toxicity (skin radionecrosis). Courdi et al. [19] delivered 6.5 Gy up to a cumulative 32.5 Gy in five fractions to the whole breast, followed by 1–3 fractions of 6.5 Gy to the tumor site, once weekly. In this study, the 5‑year local progression-free rate was 78%, with a low rate of early reactions and 52% late effects, mainly subcutaneous fibrosis. To prevent grade 4 toxicity as reported by Webb and to prevent late effects like subcutaneous fibrosis, we established treatment breaks between the fractions in our concept, so that no patient was irradiated for five consecutive days, to regenerate the healthy normal tissue and avoid higher-grade side effects [23]. A further advantage of our study is the uniform fractionation scheme applied to all patients, which facilitates a reliable assessment of this fractionation.
Nair et al. [17] also compared different concepts of breast irradiation, both in the curative adjuvant setting and for palliation. In their center, irradiation with 30 Gy in five fractions was administered to the whole breast and/or nodes, once a week, followed by a 6-Gy boost to the primary breast tumor. Acceptable local control and minimum toxicity were established.
While these concepts are similar to those described in our study, the abovementioned authors did not use a simultaneous integrated boost and, consequently, used longer overall treatment times. The advantage of our radiotherapy concept is the short treatment time and the local dose increase to the primary tumor as a simultaneous integrated boost. To the best of our knowledge, this has not appeared in the literature before.
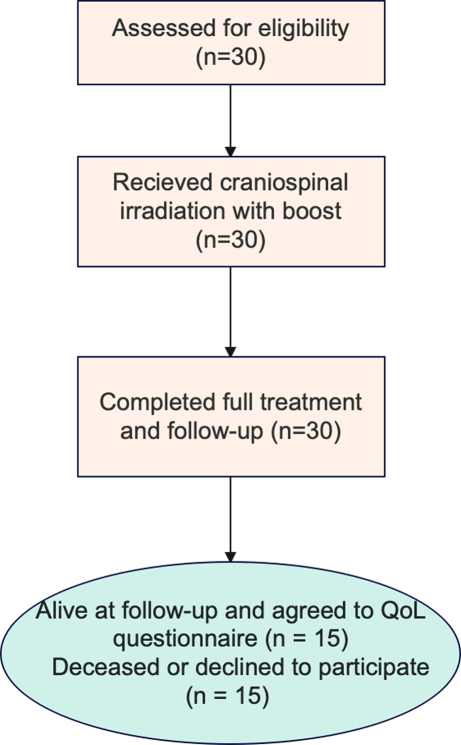
It is beneficial for elderly frail patients to complete their treatment in a short period of time. We therefore emphasize the importance of an ultra-hypofractionated approach, enabling the treatment to be completed in just one week with only five fractions. In this cohort, the overall treatment time between the first and last irradiation was 10.7 days (range 7–16 days). Many additional considerations are relevant when treating older adults in a palliative setting, such as frailty assessment and making rational treatment decisions [24].
Of all 27 patients, 9 (33%) received their first radiation treatment over 500 days after the date of initial diagnosis. These patients had already received primary anti-hormonal therapy and were irradiated with our concept in the event of local symptoms, mostly local exulceration. Of the 10 patients (37%) who were irradiated within less than 100 days of initial diagnosis, 8 had local exulceration with a high symptom burden, one was hormone receptor negative and had no options for systemic therapy due to comorbidities, and one was ineligible for systemic therapy due to general condition (ECOG 4). This explains the wide range within the patient population between initial diagnosis and first radiotherapy and shows how individually the decision is made to undergo local radiotherapy in palliative treatment regimens. The remaining patients first received systemic therapy, e.g., anti-hormonal therapy, followed by local radiation therapy in the case of symptomatic tumor burden with local symptoms.
Due to positive hormone receptors, many patients in this cohort also received systemic therapy, so the tumor responses and local control probably reflect not only the effects of local radiotherapy but also those of systemic therapies. This synergistic effect cannot be further differentiated due to the retrospective design of the study. However, since radiotherapy has been proven to be a well-tolerated temporary local treatment, it should be offered to patients as a local therapy, especially for complaints like ulceration, bleeding, and pain.
The limitations of our trial are the small number of cases and the retrospective collection of data. Furthermore, most patients had only one follow-up appointment, so late effects or re-progression were not detected in the context of our aftercare due to loss to follow-up. However, evaluating such collectives is difficult, as many patients are lost to follow-up care due to their limited general condition and the associated immobility, which makes it more difficult to assess their condition after completion of palliative radiotherapy.


Comments (0)