With the increasing aging population in society, patients with cirrhosis are also experiencing associated increase in age (Enomoto et al. 2020, 2024; Louissaint et al. 2022). The development of OHE is a significant complication of cirrhosis and the prognosis of patients with OHE is poor (Rose et al. 2020). Considering the challenges in identifying CHE in geriatric cirrhosis with physiologically impaired neuropsychiatric function, it is crucial to establish a useful and rational tool to assess the risk of OHE development in this patient group. The primary finding of the present study was that serum albumin and ammonia levels were robust factors for the development of OHE in geriatric cirrhosis. The second finding was that the sHE score, comprising only serum albumin and ammonia levels, was a useful index for predicting the development of OHE in geriatric cirrhosis.
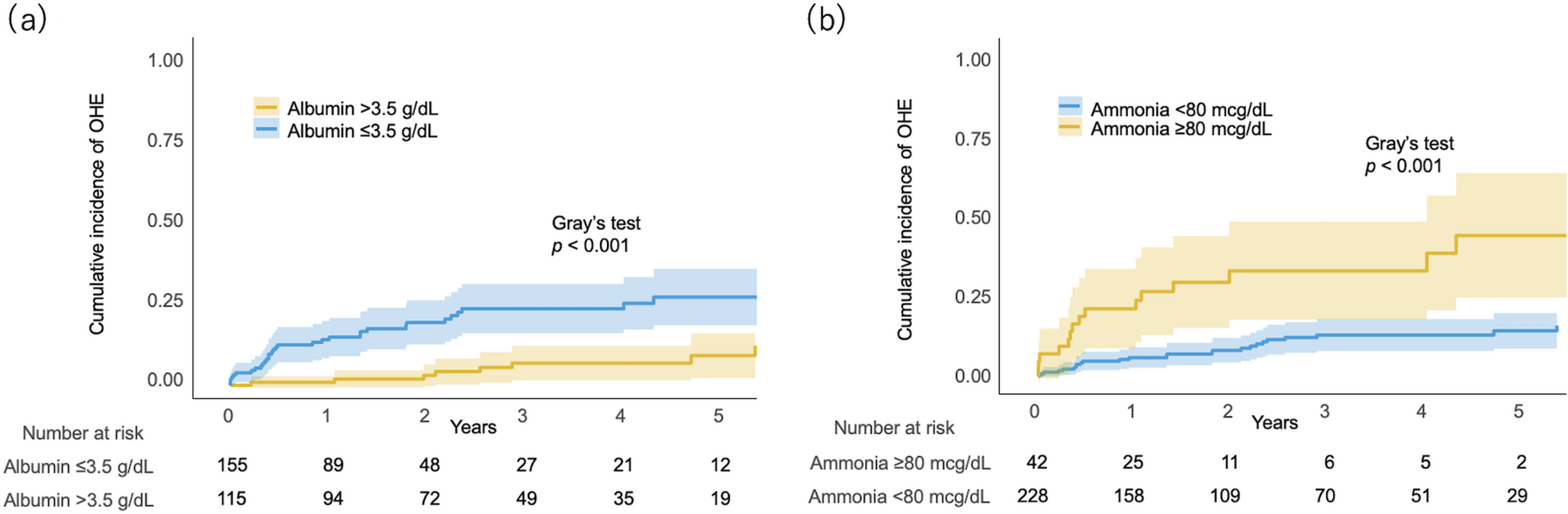
In the present study, patients with hypoalbuminemia had a 4-fold higher incidence of OHE than those with normal albumin levels. The pathophysiological role of albumin in HE can be explained by its association with inflammation. Inflammation correlates with the development and severity of HE (Claeys et al. 2021) and pro-inflammatory cytokines contribute to the development of cerebral edema, which is central to the pathogenesis of HE (Patidar and Bajaj 2015). Albumin infusion reduces inflammatory cytokines, endotoxins, and oxidative stress, and consequently improves HE in patients with cirrhosis (Wong and Loo 2023). In addition, increasing serum albumin levels by branched-chain amino acid supplementation is a promising treatment option for patients with cirrhosis associated HE (Gluud et al. 2017). The above reports support the results of the present study, indicating that serum albumin levels are a robust biomarker for the future development of OHE in geriatric cirrhosis. Indeed, serum albumin levels have been reported to stratify the risk of developing OHE in patients with cirrhosis in the United States and in Asia, which is consistent with our findings in the present study (Tapper et al. 2018; Bai et al. 2019; Miwa et al. 2022). Older patients with cirrhosis can easily develop malnutrition, which leads to protein deficiency and sarcopenia (Partridge et al. 2018). Therefore, it is essential to monitor serum albumin levels to stratify the risk of OHE and maintain it to improve the outcomes of older patients with cirrhosis.
In addition to hypoalbuminemia, hyperammonemia also plays an important role in the pathogenesis of HE. In the present study, patients with hyperammonemia had a 4-fold higher incidence of OHE than those within the normal range. Hyperammonemia contributes significantly to the development of HE through mitochondrial dysfunction, increased oxidative stress, and astrocyte swelling (Patidar and Bajaj 2015). Elevated serum ammonia levels were identified as a risk factor for the development of OHE in a multicenter cohort study (Ballester et al. 2023). In addition, serum ammonia levels are useful in predicting not only OHE but also hospitalization owing to other liver-related complications, including decompensated events (Tranah et al. 2022), and have a strong impact on mortality in patients with cirrhosis (Tranah et al. 2022; Miwa et al. 2024). In contrast, ammonia-lowering therapy is an essential treatment for OHE in these patients (Ridola et al. 2020). In patients with cirrhosis, hyperammonemia is caused by intestinal production, impaired hepatic urea cycle, decreased renal excretion, inadequate muscle detoxification, and portosystemic shunt (Gallego-Durán et al. 2024). These previous studies support the results of the present study, indicating that serum ammonia levels stratify the risk of OHE in geriatric cirrhosis.
Another important finding of the present study was the identification of a simple scoring model for the risk stratification of OHE in geriatric cirrhosis. The goal in this scoring system was to create a risk stratification model based solely on blood tests, using easily memorable cutoff values. In the present study, serum albumin and ammonia levels were independent factors for OHE development in geriatric cirrhosis, and the sHE score, composed of these factors, was also shown to be useful for predicting OHE development in the geriatric population. Several studies have reported that inclusion of serum albumin levels in scoring models is effective in predicting OHE development in patients with cirrhosis (Tapper et al. 2018; Labenz et al. 2019; Gil-Gómez et al. 2021). Furthermore, the combination of serum albumin and ammonia levels with other clinical variables can improve the prediction model for the development of OHE (Ballester et al. 2023). Although these models have a favorable ability to identify OHE development, they use complex scoring formulas for assessment and have limited clinical use in daily practice. Compared with these scoring systems, the advantages of the sHE score lie in its accessibility and memorability, allowing immediate decision making in daily practice. In particular, the incidence of OHE was notably low in patients with an sHE score of 0. As the risk of OHE development increases in geriatric cirrhosis patients with an sHE score ≥ 1, patients with either hypoalbuminemia or hyperammonemia require careful follow-up for HE. Of note, the MELD score did not predict OHE occurrence in our study and the ability of sHE score consisting only of biochemical parameters were better than ascites which requires medical imaging. Although the BABS score is a reliable indicator of OHE development, there was a marked imbalance between sensitivity and specificity with the predetermined cutoff value may be effective to stratify those with worse liver functional reserves (Tapper et al. 2018). Given its simplicity, the sHE score is an effective tool to stratify the risk of OHE in geriatric cirrhosis.
The present study acknowledges a few limitations. First, because this study focused on patients with cirrhosis in a specific region, the results may not be generalizable to other regions. Second, because this was a retrospective study, the possibility of bias cannot be entirely excluded. Third, female sex was identified as an independent risk factor for the development of OHE in geriatric cirrhosis, which is inconsistent with findings from a large cohort study (Tapper et al. 2018). The inclusion of only geriatric patients may have introduced a selection bias that affected the results of our study. Lastly, unmeasured variables and the treatment of HE may have potentially influenced the development of OHE in our study. Therefore, further prospective studies are necessary to verify the results of this study. However, we believe that the impact of these limitations is minimal because this study was conducted by reviewing a prospectively collected dataset comprising a sufficient number of patients, enabling a robust multivariable analysis.
In conclusion, the present study demonstrated that serum albumin and ammonia levels are associated with the development of OHE in geriatric cirrhosis. The sHE score is a useful index for predicting OHE development in older patients with cirrhosis. Further studies are required to provide a definitive solution to improve the impact of HE on geriatric cirrhosis..





Comments (0)