This study reveals how conflict functions not only as a source of physical destruction but also as a weapon that systematically paralyzes healthcare services. These documented experiences of civilians in Gaza who were unable to access emergency medical care and were consequently evacuated to Türkiye represent not only a public health crisis but also a direct violation of the rights to life and health. Participants’ reports suggest a perception that healthcare infrastructure was deliberately targeted and that EMS may have been obstructed or withheld as part of the conflict dynamics. Such practices align with the concept of “medicide,” a term used in literature to describe the strategic use of healthcare disruption as a tool of war [12].
The mean age of participants was 26 years (range: 18–46), which is significantly lower than the mean age of 68 reported by El Jabari et al. (2024) [13]. This discrepancy can be explained by the inclusion in this study not only of oncology patients but also trauma victims. A considerable proportion of participants required emergency care for either malignancies or extremity trauma. These findings indicate that under wartime conditions, the demand for emergency healthcare extends beyond acute injuries and includes chronic, complex, and long-term conditions that also require urgent medical attention. Indeed, Mohammed et al. (2024) reported that nearly 2,000 patients in Gaza lost access to treatment following the closure of the territory’s only oncology hospital due to fuel shortages [1].
The WHO defines equal, continuous, and unimpeded access to healthcare as a fundamental human right. However, a study by Bouquet et al. (2021) found that oncology patients in Gaza face not only barriers within their own healthcare system but also substantial obstacles in obtaining the required official permits from Israeli authorities for medical referrals abroad [14]. Among 655 patients included in that study, most initial applications were either denied or delayed, and only 386 were approved. The average delay in reaching the hospital for those approved was 77 days, which had severe adverse effects on disease progression, pain management, treatment continuity, and mental health. Similarly, our findings revealed that patients with comorbid conditions were more likely to report prolonged waiting times for ambulance services and ED access. While this suggests a potential association, the direction of this relationship remains unclear and causality cannot be inferred. Correlation analysis also showed that participants who remained longer in Gaza tended to have longer treatment durations in Türkiye. These findings suggest that access to emergency care in conflict settings may influence treatment outcomes and perceived survival chances.
Socioeconomic inequalities are among the key determinants that shape access to healthcare in conflict settings. In our study, individuals with a monthly income below 500 USD reported significantly more barriers to accessing care compared to those earning more than 500 USD per month, a finding consistent with previous research suggesting that low-income refugee populations may face limited access to healthcare and medication [1, 15]. Furthermore, several participants reported experiencing financial hardship during the referral process. Additionally, individuals with comorbidities experienced significantly longer ambulance wait times and delays in emergency department admissions compared to those without comorbidities. These results suggest that economic disadvantage and medical complexity may jointly contribute to difficulties in accessing emergency care, as perceived by participants.
The most frequently reported access barriers included the deliberate targeting of healthcare facilities, ambulance shortages, and the lack of medical supplies. Participants’ responses reflect not only the perceived fragility of the health system, but also a belief that healthcare infrastructure may have been intentionally undermined as part of the broader conflict. Studies by El Jabari et al. (2024) and Wispelwey et al. (2024) have clearly documented that such practices aim to collapse the Palestinian healthcare system [13, 16]. Consistent with these reports, our findings show that patients in Gaza were unable to receive adequate care due to the collapse of healthcare services, lack of advanced diagnostics and treatment, and shortages of medical equipment and medications, necessitating their evacuation and referral to Türkiye.
A considerable number of patients indicated that they had never received ambulance services, while many reported being unable to reach hospital emergency departments. Notably, nearly half of the participants recounted witnessing multiple deaths they believed were associated with the lack of access to emergency healthcare. These self-reported observations suggest that perceived deficiencies in access may be associated with fatal consequences; however, due to the study’s design and measurement limitations, causal relationships between healthcare access and mortality cannot be established. This aligns with the findings by Nelson et al. (2005) and Venugopal et al. (2007) that underscored the life-threatening consequences of inadequate access to emergency medical care during armed conflict [17, 18].
One of the most commonly reported structural barriers during the international referral process was the language barrier, because many international humanitarian workers did not speak Arabic. This impeded effective communication between healthcare professionals and patients, disrupting diagnostic accuracy, treatment planning, and in-hospital navigation. In a study focused on refugee populations, Cansızlar and Beydağ (2022) also emphasized that language limitations create uncertainty in clinical decision-making, jeopardize patient safety, and directly reduce the quality of healthcare services [19]. Therefore, healthcare teams serving patients evacuated from conflict zones must work with qualified interpreters to ensure clinical effectiveness and uphold ethical standards.
Many participants reported experiencing complications due to insufficient medical care. These complications often involved inadequate treatment in hospitals, the development of infections, and resulting clinical conditions such as amputations that led to permanent disabilities. Similarly, Aldabbour et al. (2024) reported that the shortage of specialized healthcare personnel and essential medical equipment in Gaza significantly hindered the optimal management of trauma and neurological cases [20]. In the present study, deficiencies such as lack of medical staff, shortages of medications and equipment, the unavailability of hospital beds, and frequent power outages were frequently perceived by participants as contributing to poor treatment and recovery experiences.
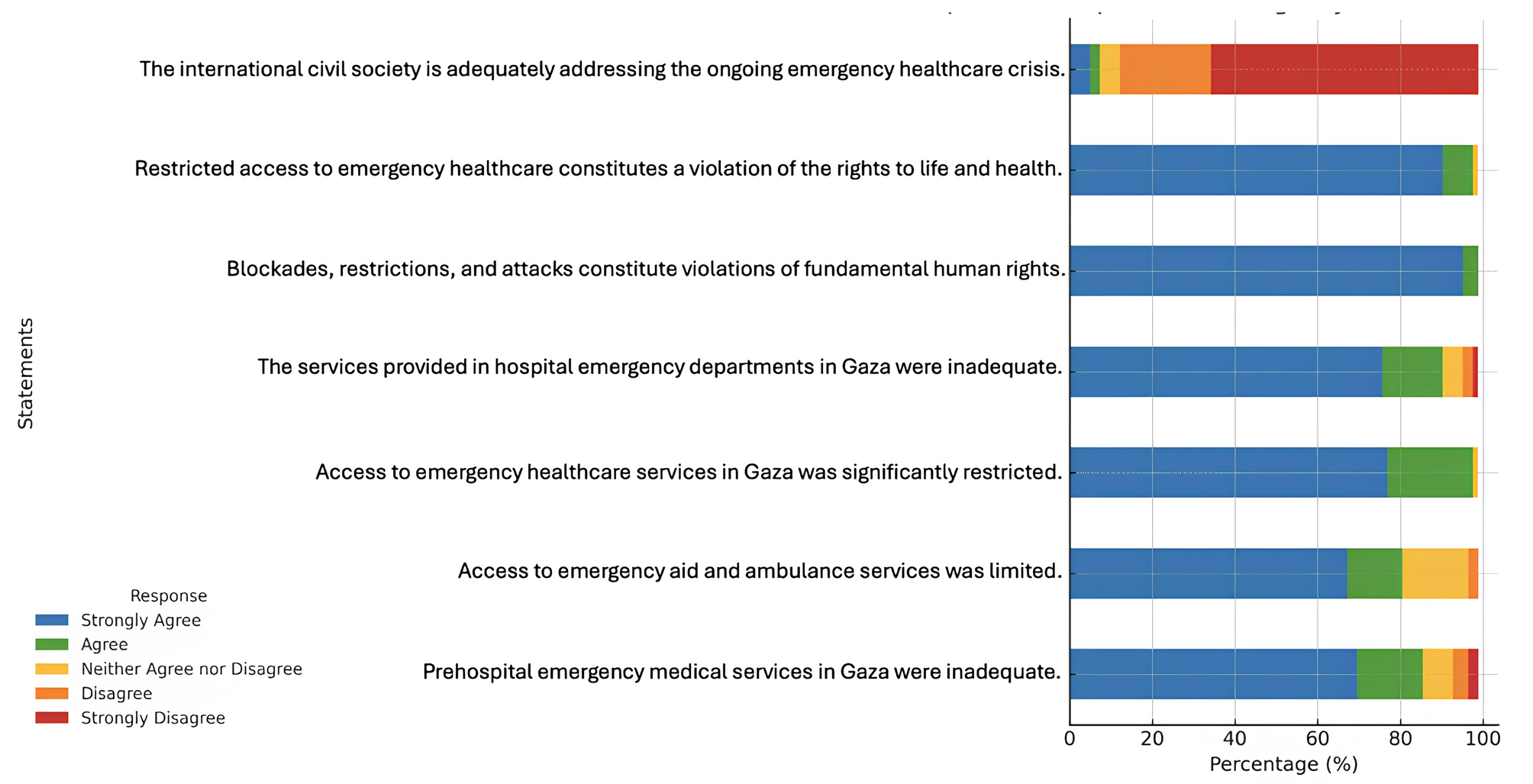
A considerable number of participants expressed dissatisfaction with the international community’s response to the health crisis in Gaza. This perspective is not limited to individual opinions; Beiraghdar et al. (2023) also highlighted the limited visibility and ineffectiveness of interventions by international organizations such as the WHO and the United Nations (UN) in addressing the multifaceted humanitarian crisis in Gaza [2]. The inaction of international mechanisms in safeguarding health services during wartime creates an environment where violations of civilians’ fundamental health rights remain largely invisible and unpunished.
In this context, a considerable proportion of participants reported violations of the right to life, and the right to health. Notably, a portion stated they were directly attacked within hospital settings, underscoring that the conflict extends beyond the front lines into healthcare facilities themselves. Studies by Levy et al. (2024) and Hamshari et al. (2024) have described the obstruction of access to healthcare in Gaza as a clear breach of international humanitarian law [21, 22]. In our study, a substantial proportion of participants called for Israel to be prosecuted in international courts, while most believed the WHO should be held accountable for documenting Israel’s obstruction of healthcare access. These responses appear to reflect not only individual outcries but also a concrete call for accountability grounded in international humanitarian law. Supporting this, Venugopal et al. emphasized that safeguarding healthcare services during war and disasters is not solely the responsibility of nation-states, but also a principal obligation of international organizations [18].
Although the psychosocial conditions of patients with malignancies should also be assessed, in a context where even basic medical access is largely unattainable, the need for psychological support has become secondary. In conclusion, this study comprehensively illustrates the inequalities in healthcare access during wartime and the destructive impact of conflict on healthcare systems. When interpreted alongside with literature, our results highlight that protecting EMS and implementing specialized health policies for war victims are not only ethical and humanitarian imperatives but also legal obligations [1, 15]. Although this study primarily focused on physical health access barriers, the profound psychological distress experienced by patients—including trauma, anxiety, and uncertainty—warrants further investigation in future research.
These findings offer several actionable insights for improving access to emergency medical care in conflict zones. First, the deployment of mobile field hospitals may address local infrastructure collapse. Second, multilingual healthcare teams or trained interpreters should be included in international missions to overcome language barriers. Third, international organizations must enhance coordination for medical evacuations and ensure neutral monitoring of access violations. Lastly, legal accountability mechanisms must be established to document and respond to systematic obstruction of healthcare services. These measures can help bridge the gap between humanitarian principles and real-world practice in war-affected regions.
Limitations
While this study provides critical insights into access to EMS in a conflict setting, it is subject to several methodological limitations. First, the research exclusively includes patients who were medically evacuated to Türkiye and treated at a specific healthcare institution. Consequently, the experiences of individuals who remained in Gaza or received treatment in other countries are not represented, which limits the generalizability of the findings. These individuals likely represent a specific subset of patients who were eligible and prioritized for international evacuation, which may not reflect the broader population affected by the conflict.
Second, since the data rely on participants’ self-reports, the objectivity of responses may be partially influenced by post-traumatic cognitive effects or potential recall bias. Third, the use of interpreter assistance in some interviews may have led to semantic distortions or nuanced discrepancies in language translation. Moreover, although the study includes analytic comparisons, its cross-sectional design, measurement limitations, and non-representative sample preclude any causal interpretations. The findings should therefore be considered exploratory and hypothesis-generating, offering a descriptive snapshot of conditions during a specific period. Additionally, the study lacks baseline or pre-conflict data, limiting the ability to assess how access barriers evolved over time or differed from pre-war healthcare conditions.
Furthermore, although the questionnaire was developed with expert consultation and piloted for clarity, no formal psychometric validation (e.g., internal consistency or reliability testing) was conducted, which may affect measurement precision.
Lastly, the analysis was limited to univariate and bivariate comparisons due to sample size constraints. The lack of multivariable modeling restricts the ability to adjust for potential confounders such as age, sex, comorbidities, or socioeconomic status.



Comments (0)