To our knowledge, this is the first study that analyzed the pattern of antibiotic consumption in Western China according to the AWaRe framework, which covers 83% of public health institutions in Sichuan province, including tertiary, secondary, and primary health institutions. It provides the basic characteristics of antibiotic usage in this province and identifies deficiencies and significant regional differences in antibiotic consumption.
There are several important findings of antibiotic consumption patterns in Sichuan Western China. First, the proportion of Access antibiotic consumption was lower than in other countries around the world and fails to meet the WHO target of at least 60% of access antibiotic consumption, though it is at a moderate level compared to other regions in China. In this study, the proportion of Access antibiotic consumption was 46.83% in Sichuan, which was higher than the national estimate of China in 2015 (33.3%) [9] and other provinces in China (Shanxi 40.31% [24], Shandong 45.2% [17]), but still lower than the global average of 60.6% at 2015 [9], the median percentage (68%, range: 22–77%) of 8 high-income countries at 2018 [25] and that in some developing countries, such as 80.3% in public sector of Limpopo province, South Africa [26], 64.8% in Sierra Leone [27]. The Chinese government has established a comprehensive system for antimicrobial stewardship in healthcare institutions [28,29,30], which produced significant achievements, including the reduction of antibiotic consumption and the reduction of irrational drug use [31,32,33]. However, this study showed that the proportion of Access antibiotic consumption was not yet achieved the target of WHO, indicating that further exploration is needed to identify the reasons for this result and to develop targeted strategies for improving the patterns of antibiotic consumption.
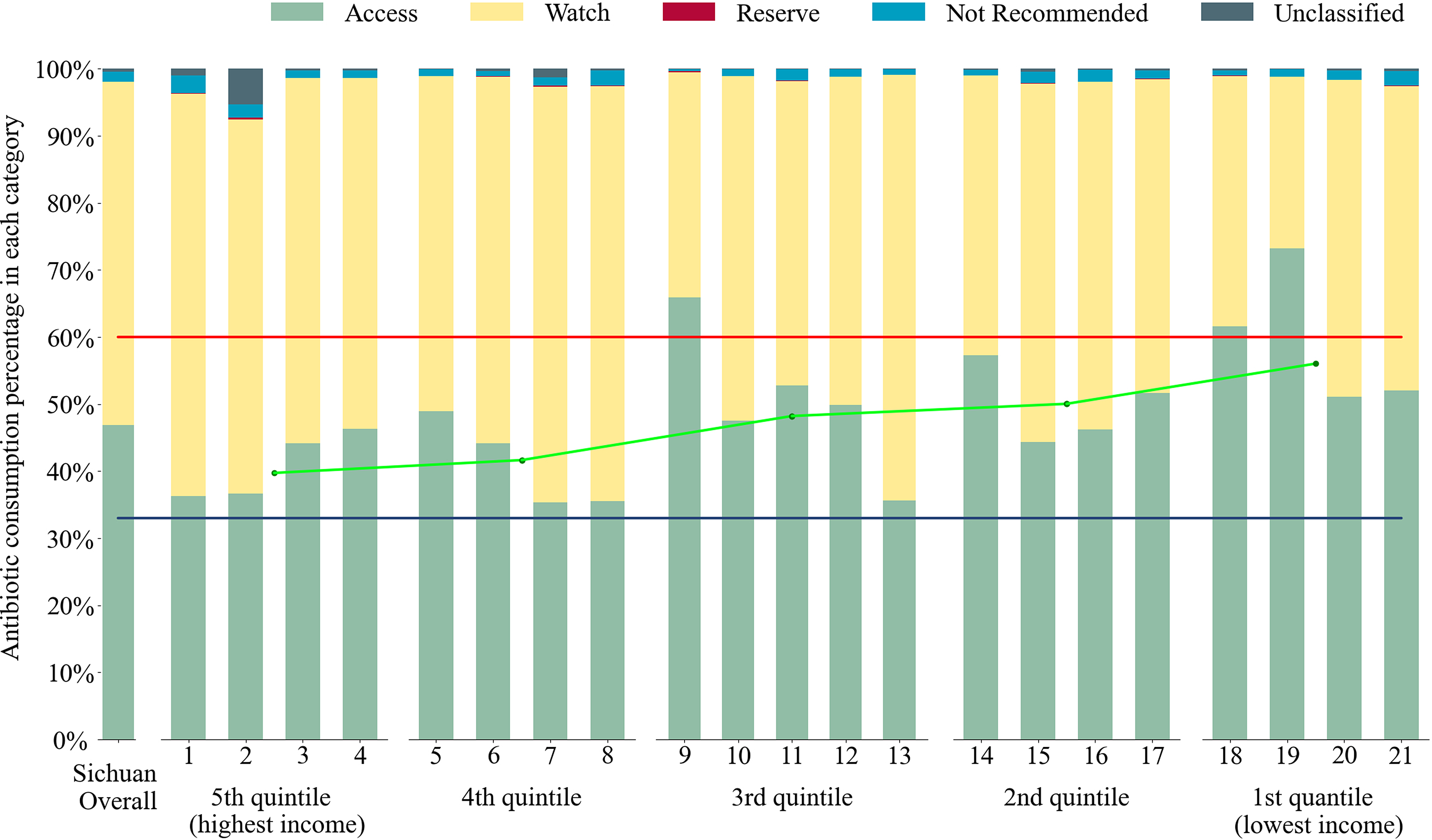
There may be several reasons why the proportion of Access antibiotic consumption was relatively low in China. First, the antibiotics management classification system in China was different from the WHO AWaRe classification. In China, antibiotics were classified into unrestricted, restricted, and special management categories, and prescription of restricted and special antibiotics was limited so as to improve the rational use of antibiotics [34, 35]. However, as shown in Fig. 2, approximately 10% of total antibiotic consumption, which was classified as WHO Access antibiotics, was categorized as restricted antibiotics; and approximately 35% of total antibiotic consumption, which was classified as WHO Watch antibiotics, was categorized as unrestricted antibiotics in China. This difference may influence the achievement of WHO’s target. Therefore, communication and coordination of the two systems are warranted to align the international and national efforts to improve the pattern of antibiotic consumption, with an appropriate monitoring and feedback system and mechanism.
Second, inappropriate antibiotic prescribing has been highly prevalent in China [36]. Several factors may contribute to this phenomenon, including the misperception of patients who regard antibiotics as a panacea and prefer higher-level (and more expensive) antibiotics, and doctors who prescribe unnecessary antibiotics to patients due to a lack of professional knowledge or wish to satisfy the patients [37]. Education on the rational use of antibiotics for doctors should be valued and encouraged, at least including the specifications and guidelines for infectious diseases. In addition, publicity on antibiotic use for residents was also crucial.
There are significant regional disparities in antibiotic consumption patterns in Sichuan. Low-income regions had higher antibiotic consumption and higher proportions of Access antibiotic consumption than middle- and high-income regions (except for the highest 20% income quantile regions). This phenomenon was also observed in Shandong China [17]. However, different phenomena were observed in global research, which showed that antibiotic consumption increased gradually with the income level of countries, and the proportions of Access antibiotic consumption were similar between high-, up-middle, and low-middle income countries in 2015 [9].
The regional disparities may be caused by multiple factors. First, regions with lower income were more likely to lack qualified physicians in China, which was the biggest barrier to reducing antibiotic overuse [38, 39]. Second, the expectations of patients for antibiotic therapy in low-income regions [40] might be also important causes resulting in higher antibiotic consumption. Thirdly, the weak supervision and a large number of inappropriate antibiotic prescribing in primary health institutions exacerbated antibiotic overuse in low-income regions. Antibiotic stewardship primarily targeted urban tertiary and secondary hospitals instead of primary health institutions during past during the past decade and more than 70% of antibiotic prescriptions were inappropriate in institutions healthcare facilities in China [30, 41]. On the other hand, mobile visits of patients might be the reason why antibiotic consumption in the highest 20% income quantile regions was higher than in the 2nd 20% income quantile regions. Mobile visits of patients from low-income regions to high-income regions for higher-quality treatments were becoming increasingly common [42], which led an overestimation of antibiotic consumption based on population in high-income regions.
Overall, in high-income regions, the problem of underuse of Access and overuse of Watch antibiotics was more serious than its counterparts. While in low-income regions, antibiotic overuse was more prominent, where it was urgent to take measures to curb antibiotic abuse, such as educating patients and physicians on antibiotic use and enlarging the scope of antibiotic stewardship to cover primary health institutions.
The strength of the study lies in the use of hospital drug consumption surveillance data. Several data sources have been used to examine the antibiotic use pattern, including the point prevalence survey data [15] which may not reflect use patterns over a period of time, and drug sales data which may not reliably reflect actual consumption [9]. The hospital drug consumption surveillance data involving nearly all public hospitals and primary health institutions in a vast region in a whole year, providing a more comprehensive and accurate estimate of antibiotic usage patterns than other data sources. Second, the consumption of antibiotics group was calculated according to the internationally recognized WHO AWaRe classification system, which enabled national and international comparisons for problem identification and strategic planning for improvement.
This study has several limitations. First, due to the limitation of the data source, only public health institutions were included, and data from private medical institutions and private pharmacies were lacking in this study. Therefore, the total consumption may be underestimated. However, as public health institutions are the dominant providers of healthcare in China, and weight adjustment of the population has been used, the influence may be minimal. Second, this is a cross-sectional study that examined the antibiotics consumption pattern in 2020, further study could employ longitudinal data to get more insights into the changing trend of AWaRe pattern in this region. Third, this study observed considerable regional disparities. Further studies are warranted to uncover the underlying socioeconomic and health system determinants so that tailored strategies considering local characteristics could be made to promote rational use of antibiotics at the regional and county level.



Comments (0)