
Remember me
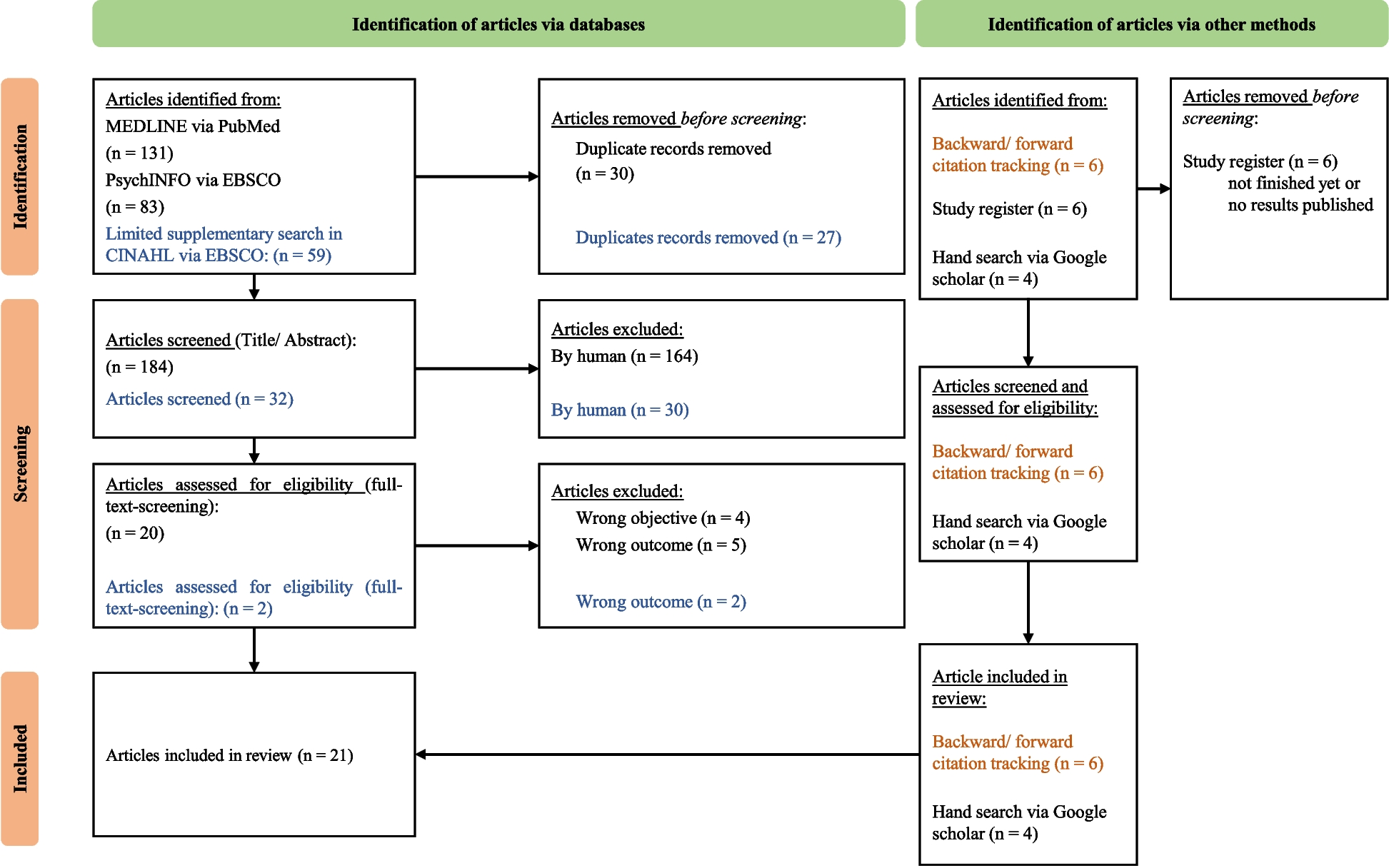


The systematic literature search in PubMed, PsychINFO, and CINHAL resulted in 273 records, which were reduced to 216 after removing duplicates. These were screened in the following title-abstract screening, where 22 articles were identified for the full-text screening. In addition, five ongoing trials were identified from trial registries. These studies were excluded because they were ongoing trials with no published study protocol or results. Additionally, six articles were eligible from backward and forward citation screening and four from a hand search via Google Scholar. In the end, a total of 21 studies were included for data extraction and analysis (see Fig. 1).
Fig. 1 Study characteristics
Study characteristicsThe majority of the studies were conducted in Europe (N = 11) and North America (N = 7) in the early phase of the COVID-19 pandemic (2020–2021). They were designed as empirical studies with a quantitative approach (N = 14). Most of the studies were published in 2022 (N = 5). Six studies were planned between 2020 and 2023 and published as study protocols. Furthermore, one study was published as a concept paper. The study characteristics are available in Table 3.
Table 3 Characteristics of the included studies (N = 21)Intervention characteristicsIn total sixteen interventions for nurses and physicians were explored. Nine of these are categorized as ‘evidence-informed’, which means that these PTSD-interventions are modified or new developed during the COVID-19, but without an existing proof of effectiveness. Of the sixteen interventions, four were identified as evidence-based, as their effectiveness had been evaluated in dedicated studies.
Further, five interventions were delivered face-to-face, and eleven were digital.
Aims of the intervention and their theoretical approachesAll studies reported about a rationale and aim for developing an intervention, such as being aware of the need for self-care [26, 28], strengthening of resilience [26] or support for psychological well-being [27, 36, 37] of nurses and physicians. Additionally, PTSD-related interventions have the potential to mitigate the long-term mental health impacts on nurses and physicians [27, 30], and to improve symptoms of PTSD or other related disorders [34, 38]. Fogliato et al. [39] reported about a more specific intervention-based goals, like for the EMDR to “[…] restore a natural way of processing the information in the memory to achieve an adaptive resolution through the creation of new, more functional connection.” [39].
Most of the interventions are theory-driven, drawing on a model such as the Anticipate-Plan-Deter (APD) model [28], the psychoeducational model, based on Lazarus and Folkman’s transactional stress model [29, 40], the stress continuum model [30], the Adaptive Information Processing (AIP) model [39] or the RAPID model [41]. Some interventions did not use an underlying theoretical approach [27, 36, 37].
Form and modality of intervention useMany of the interventions included some form of peer support, for example, support provided by other staff, colleagues or team members. This component was used in various ways, for example, as the main component of the intervention [26,27,28, 42, 43] or as an additional component of an evidence-based intervention, such as in PFA [30] or CBT [33].
Most of the interventions were classified as ‘evidence-informed’ consists of CBT, PFA, or other components [11, 28,29,30,31, 33, 34, 38, 40, 41, 43, 44]. In contrast, four interventions are considered evidence-based and include components such as EMDR [35, 39], CBT [45, 46] or PFA [36, 37].
Other interventions are designed by integrating additional components, like a telephone-hotline or a supervision [29, 36, 37, 40]. For at least three interventions, it was not possible to determine whether they consist of evidence-based or evidence-informed components [26, 27, 42].
Most of the intervention were applied using a digital modality [27, 29, 31, 33,34,35,36,37,38, 40, 43,44,45,46,47] and by trained professionals with expertise, such as in CBT [29, 40] or CBT and mindfulness [45, 46] or PFA [35,36,37] or EMDR [35].
The duration of the interventionsDepending on the modalities used, the sessions and modules of the interventions were not fixed to a specific duration, allowing flexible use of the intervention [27, 28, 45, 46]. The developers of the interventions provided an estimated duration of each session [29, 40]. They vary from 90 min [32, 39] to 30–60 min [33, 34, 38] to 20 min [43].
Some interventions are designed as programs so that developers are able to estimate the duration of the entire intervention, which varies from one day (eight hours) [27, 41] to eight weeks [29, 34, 38, 40]. Some studies do not provide information about the duration [
Comments (0)