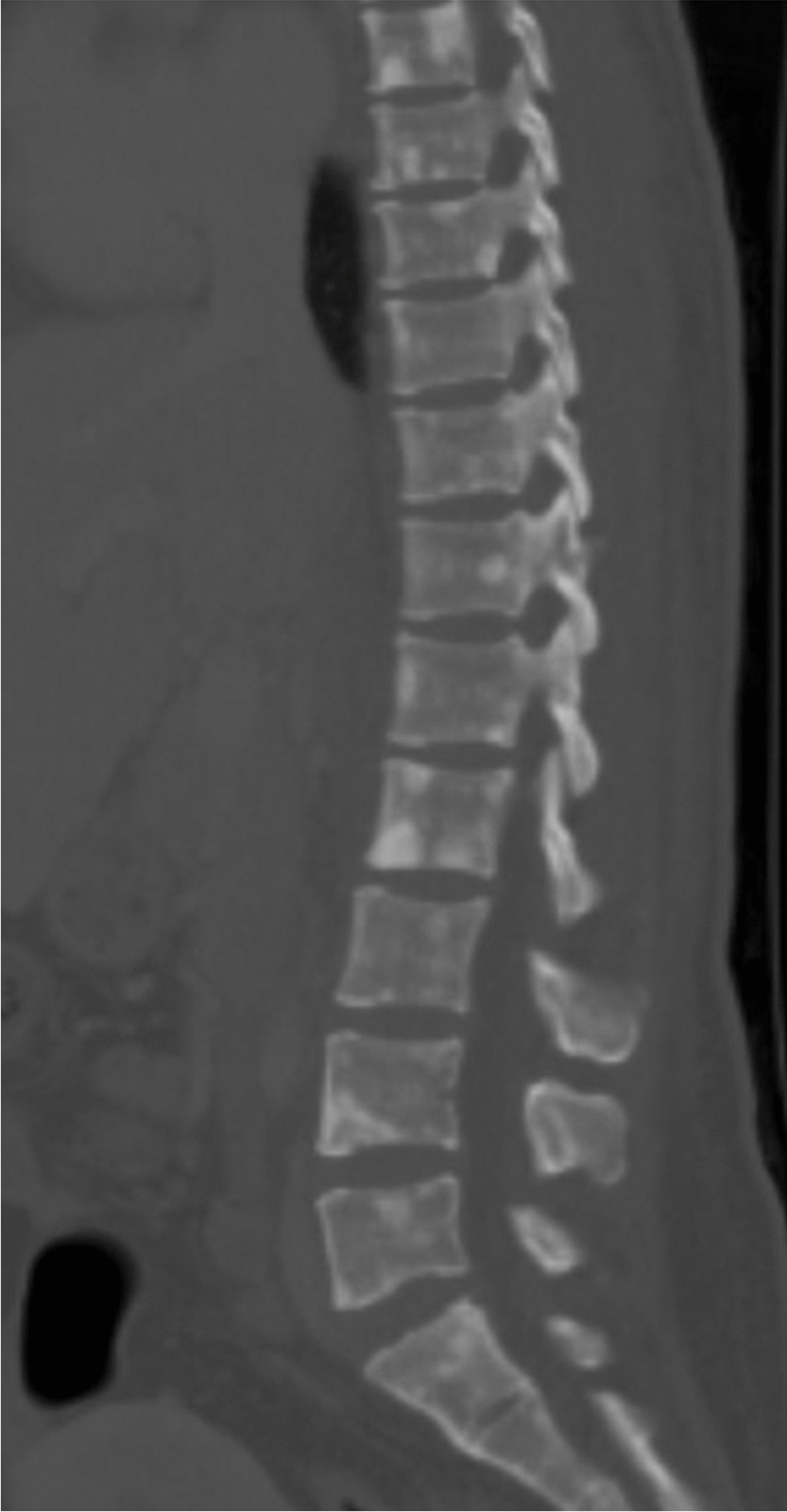
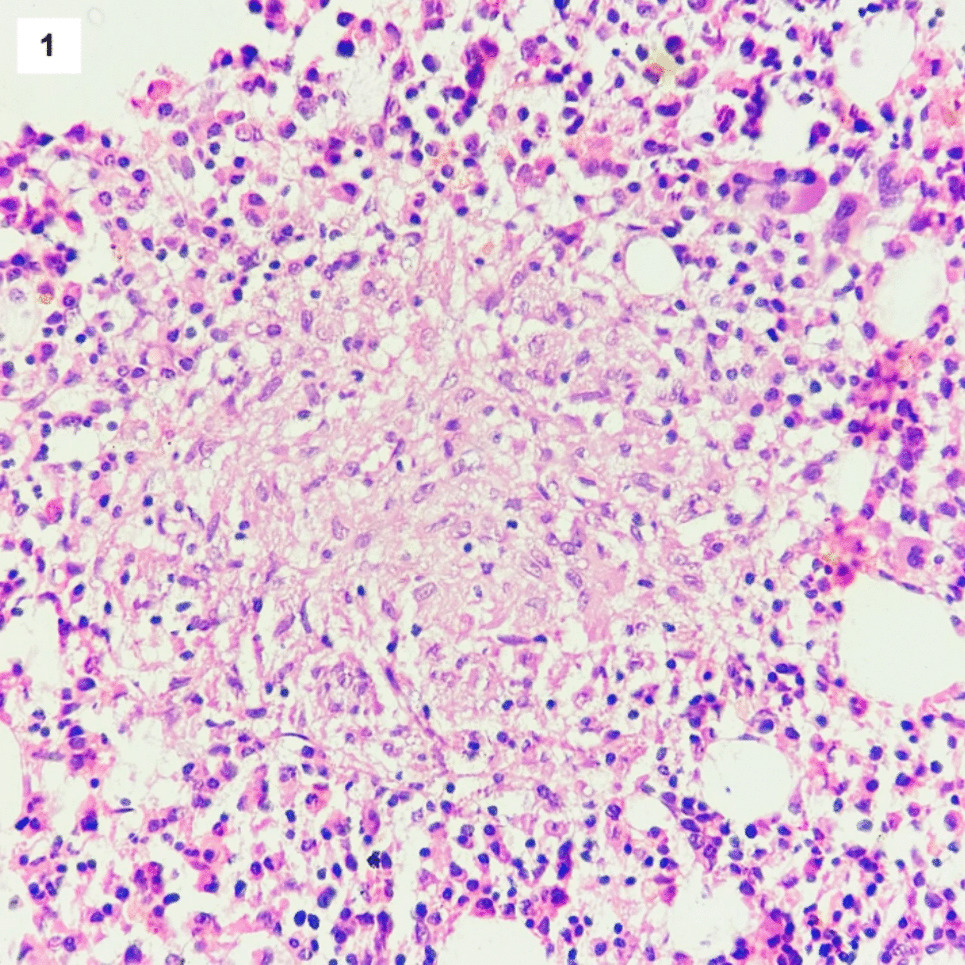
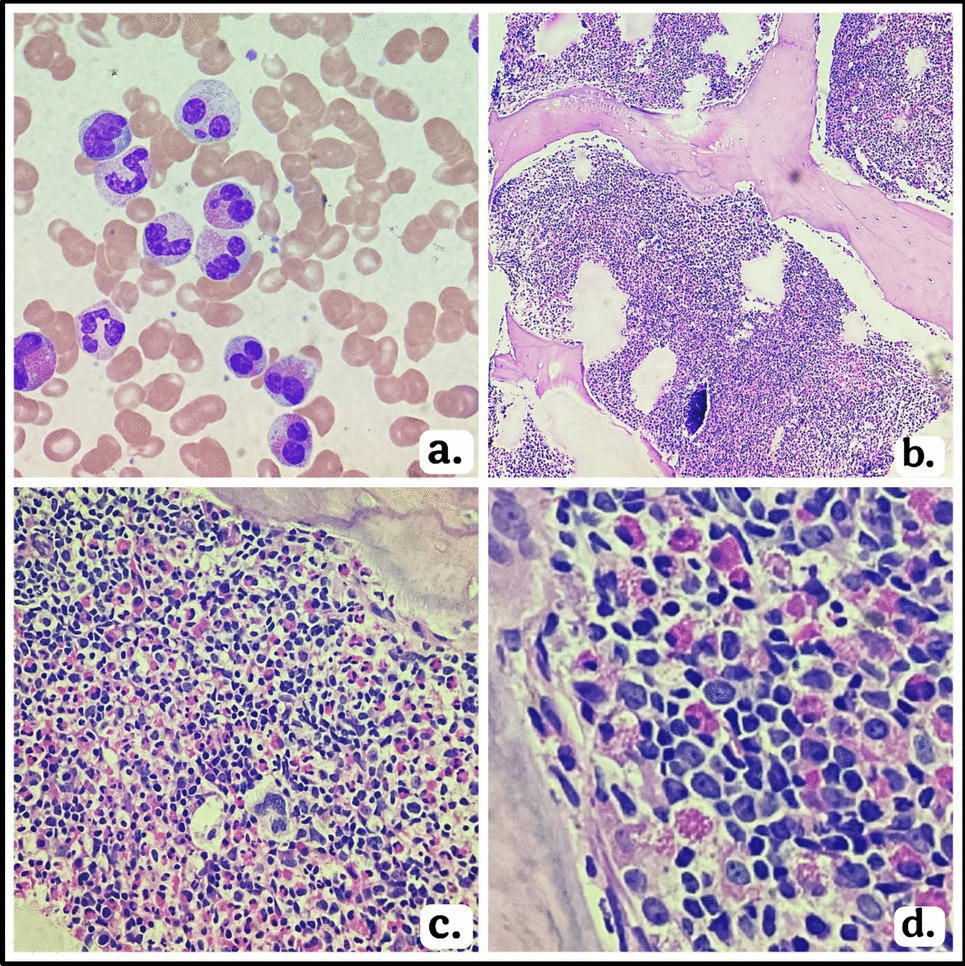
Since NSMM by definition does not have detectable IG in serum or urine, monitoring is more dependent on PET/CT and bone marrow sampling, rather than the biochemical markers [3]. Bone marrow examination, multiparametric flow cytometry for minimal residual disease, and imaging for tracking skeletal lesions are the best methods to assess response to therapy and minimal residual disease [9].
It has been proposed that NSMM may have a different prognosis compared to secretory MM, but the literature is inconclusive (see summary in Table 1.). This is complicated by the fact that methods for detecting paraproteins have changed over time, making it difficult to compare the results of different studies. Theoretically, NSMM could have a better prognosis due to the absence of light chain deposition in the kidney and other organs and the lack of immunoparesis. Conversely, the absence of detectable paraprotein may also delay diagnosis, leading to a worse prognosis. There may also be other differences in disease biology and response to therapy inherent in NSMM vs secretory MM such as the greater immunogenicity of monoclonal light chain antigens, which elicited a strong type 1 major histocompatibility complex response with T-cell mediated tumor rejection in murine models [3, 26
Table 1 Comparison of overall survival (OS) between NSMM and secretory multiple myelomaNotably, NSMM patients may be denied access to clinical trials due to the lack of measurable biomarkers which may be required by study protocols.
Smith et al. [27] reported in 1986 a series of 172 consecutively diagnosed MM in Manchester, UK, with 13 NSMM patients. Overall survival (OS) was superior in the NSMM group compared to secretory MM (46 versus 21 months, P < 0.01). However, since this study predates the sFLC assay, it is likely the “NSMM” group also included cases of OSMM.
A 2003 study by Kyle et al. of 1027 MM consecutively diagnosed at Mayo Clinic in the years 1985–1998 found no difference in the OS for 29 NSMM patients versus standard MM cases. Of note, in 5 of 29 NSMM patients, an M protein developed on follow-up [28].
Chawla revisited the Mayo data, including all patients diagnosed 01/1973–06/2012. There were 124 cases of NSMM compared to 6953 patients with “typical” MM. As noted in the Kyle study, in cases diagnosed prior to 2001, OS was similar between NSMM and secretory MM patients. However, the authors found different results when they analyzed the cohort diagnosed between 2001 and 2012, during which time novel therapies such as lenalidomide and proteasome inhibitors came into use. In these patients, OS of NSMM was significantly better than that of secretory myeloma: 8.3 years vs 5.4 years (P = 0.03), a difference that remained significant after adjusting for ISS stage [6].
A retrospective study conducted in China by Qin et al. on newly diagnosed MM cases treated with either bortezomib-based or thalidomide-based therapy analyzed MM with unmeasurable M protein (categorized as 61 OSMM, 19 NSMM, and 7 non-producer MM cases). Patients with NSMM had a lower International Staging System (ISS) disease, while those with OSMM showed a higher prevalence of renal dysfunction as compared to the other groups. Plasma cells in cases categorized as non-producers were noted to predominantly have plasmablastic morphology, and these patients were significantly shorter than the other groups (median OS 2.0 months compared to 22.0 for NSMM, 30.0 for OSMM, and 51.0 in measurable disease). NSMM and OSMM had shorter progression-free survival (PFS) and OS than secretory MM, an association that remained significant in multivariate analysis (PFS hazard ratio 2.190; P < 0.001, OS hazard ratio 2.441, P < 0.001) [29].
Interestingly, when comparing drugs received, bortezomib versus thalidomide, survival was significantly better in patients treated with bortezomib in secretory MM, but there was no difference in survival based on treatment in the non-measurable disease group. The authors speculate this could be due to non-measurable MM cells having levels of IG too low to activate the unfolded protein response (UPR), which is the target of bortezomib [29].
A study of 852 consecutively diagnosed MM in Athens, Greece, and Tel Aviv, Israel, contained 110 OSMM and 20 NSMM patients. NSMM patients tended to be younger, have less anemia, and have lower ISS compared to secretory, but similar 4-year OS. OSMM showed better overall survival (4-year OS of 64% vs 58, P = 0.034). However, the OSMM group had lower bone marrow plasma cell infiltration, rates of anemia and hypercalcemia, and ISS stage compared to secretory disease. There was no difference in OS between OSMM and NSMM compared to secretory MM in multivariate analysis adjusting for ISS stage, age, LDH, and high-risk cytogenetics [10].
A study published by Wålinder et al. in 2020 compared survival in 4325 MM patients in the Swedish Myeloma Registry. Secretory MM was compared to non-measurable disease (OSMM and NSMM) [7]. Nine percent of their patients had non-measurable MM, 6% OSMM, and 3% NSMM. There were no statistically significant differences in OS between secretory MM, OSMM, and NSMM. Statistically significant associations included lower ISS stage for OSMM and NSMM, lower percentage of bone marrow plasma cells, and lower creatinine compared to secretory MM. In multivariate analysis, younger age (< 65 years versus ≥ 75 years) was associated with superior survival in OSMM, while low stage and autologous stem cell transplant remained significant for survival in NSMM [7].
Nandakumar et al. reported on Mayo Clinic patients, finding 30 NSMM patients diagnosed from 2008 to 2018. These were compared to a control group of 60 newly diagnosed MM. Contrasting with the other reports, the NSMM patients in this cohort were noted to have a higher tumor burden and higher rate of ISS stage III [30]. Median OS for NSMM was worse than the control group (59 vs 92 months), but this was not statistically significant (P = 0.257). The most common genetic abnormality in NSMM was t(11;14) (almost 60% of cases), as had been observed by Qin et al. in OSMM and NSMM [29]. The NSMM bearing this translocation had a statistically significant shorter OS (46 months versus 64 months, P = 0.003) compared to NSMM cases without this translocation [30].
Sun et al. recently performed a large multicenter retrospective study on NSMM, enrolling 176 NSMM patients in China, and found that the OS difference was not statistically significant between those patients and a control group of secretory MM [31]. Unlike the Nandakumar study, NSMM more often had low ISS stage compared to the control group.
Given the current evidence, the International Myeloma Working Group states that the treatment, response to therapy, and survival rates of NSMM patients are similar to those in secretory MM [8]. Therapy for NSMM is currently the same as for secretory MM.




Comments (0)