Patients
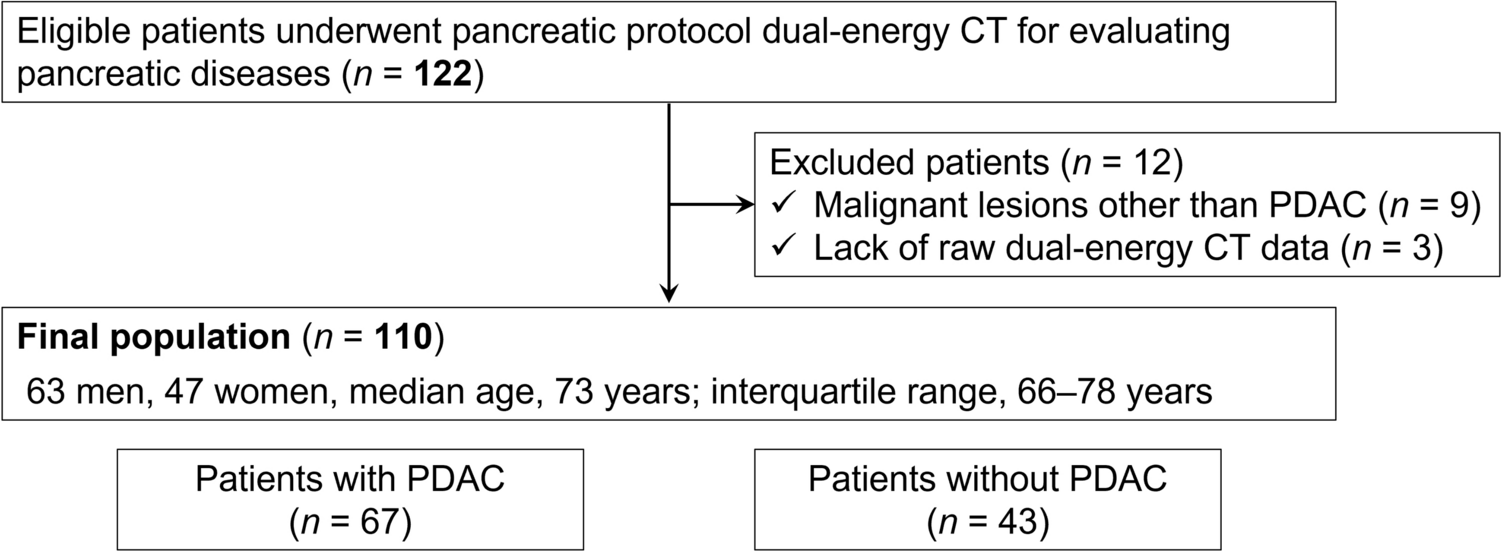
This was a retrospective study approved by our institutional review board, and written informed consent was waived. Data generated by the authors or analyzed during the study are available at Gifu University Hospital. Between February 2019 and May 2023, 122 consecutive patients with known or suspected pancreatic disease based on previous CT examinations, clinical symptoms, and/or blood test values who underwent pancreatic protocol DECT were identified. The inclusion criteria are adult patients (≥ 18 years) and scanned by Revolution CT with Apex edition (GE HealthCare). The exclusion criteria were patients who have severe pancreatic atrophy, receive reduced contrast material dose, or have malignant lesions other than PDAC, and lack of raw DECT data.
Dual-energy CT technique and contrast injection
All examinations were performed with a rapid kilovoltage-switching DECT scanner (Revolution CT with Apex edition). The pancreatic protocol DECT imaging parameters were tube voltage (80/140 kVp), noise index (7.0 Hounsfield unit; HU) at 5-mm slice collimation based on adaptive statistical iterative reconstruction-Veo of 40%, tube current (variable; GSI Assist; GE HealthCare), detector configuration (128 detectors with 0.625-mm-section thickness), beam collimation (80 mm), rotation time (0.5 s), pitch (0.581:1), scan field of view (large body), and display field of view (38 cm). The raw DECT data at 1.25-mm-section thickness with 50% overlap were reconstructed adaptive statistical iterative reconstruction-Veo of 40%. Reconstructed images at 1.2-mm thickness in the coronal plane were also available.
Intravenous iodinated contrast material containing a 300-mg iodine per milliliter (iopamidol, Iopamiron 300®, Bayer HealthCare or iohexol, Omnipaque 300®, GE Healthcare Pharma) adjusted for the patients’ body weight (600 mg of iodine per kg) was injected over a fixed duration of 30 s. Real-time fluoroscopic monitoring scan (140-kVp, 10 mA) was initiated 10 s after administering contrast injection. Diagnostic CT scans were performed with additional delays of 20 and 60 s for the pancreatic and portal venous phases, respectively, after a bolus-tracking program (SmartPrep; GE HealthCare) detected an 80-HU threshold in the abdominal aorta.
Identification of the optimal material decomposition images
The DECT images were transferred to Advanced Workstation server 4.7 (GE HealthCare). Twenty-seven materials were used for reconstructing MD image datasets after installing mass attenuation coefficient csv file of all materials which were provided by the vendor (Table 1). One MD image dataset consists of two materials, each of which has an opposite combination. Therefore, a total of 702 (27 × 26) image datasets were obtained for the final patient cohort.
Table 1 Materials used for reconstructing material decomposition image datasetsA study coordinator (Y.N., with 12 years of experience in abdominal radiology) placed circular regions of interest (ROIs) on the normal pancreas and PDAC on the pancreatic phase 50-keV VMIs in the patients with PDAC. For the normal pancreas, the ROI was placed at a spared portion of pancreatic parenchyma in patients with PDAC at the head/uncinated process or a downstream segment from PDAC in patients with PDAC at the body/tail. For PDAC, the ROI was placed as much of the lesion as possible on images showing the maximum PDAC diameter while avoiding artifacts and large vessels. The ROI placed on the 50-keV VMIs were automatically transferred to a similar location on the other VMIs datasets at 40-, 45-, 55-, 60-, 65-, and 70-keV levels and all 702 MD image datasets.
Subsequently, the contrast difference between normal pancreas and PDAC was calculated using the following equation: contrast difference = [(CT attenuation or concentration of normal pancreas − those of PDAC)/CT attenuation or concentration of normal pancreas] × 100 (%). The top three image datasets showing maximum contrast difference were selected, and then, four radiologists selected the best one based on the z value and image quality for diagnostic acceptability in consensus. The z value is a statistical measurement that describes the relationship between the mean value and standard deviation (SD) and normalizes the measurements with consideration for not only the mean value but also variability. The greater absolute figure of the z value represents higher mean value and less variability with stability compared to the small absolute figure of the z value.
Image analysis
The pancreatic phase iodine-based (Iodine/Water) images and 50-keV VMIs (conventional image dataset) and the pancreatic phase optimal MD images and 50-keV VMIs (optimal image dataset) were independently reviewed in a random order by four radiologists who are different from four radiologists mentioned in the previous section, which included two expert radiologists (T.K. and N.K., with 6 and 11 years of experience in abdominal radiology, respectively [expert]) and two trainees (M.H. and A.I., with 1 and 3 years of experience in radiology [trainee]) blinded to clinical information, material pair’s name, and final diagnosis. The preset window settings for the 50-keV VMIs were fixed at 490-HU width and 90-HU level [17], those for the iodine-based images were fixed at 150-HU width and 50-HU level (GE HealthCare’s default setting), and for the optimal MD images identified were fixed at 1,500-HU width and – 550-HU level (lung window). The radiologists were allowed to adjust the window settings at their own discretion during the interpretation.
The radiologists independently graded the presence or absence of PDAC using a five-point scale [4]: 5, definitely present (unequivocal visualization of PDAC distinct from surrounding nontumorous pancreas); 4, probably present (likely presence of an indistinct PDAC along with secondary features such as duct cutoff); 3, equivocal (indistinct PDAC may be present and secondary features such as duct cutoff are lacking); 2, probably absent (poor visualization of pancreatic mass from surrounding nontumorous pancreas); and 1, definitely absent (no pancreatic tumor identified). A confidence rating of 3–5 was considered indicative of the presence of PDAC.
Reference standard for PDAC
All PDACs were confirmed by ultrasound-guided fine-needle aspiration and pathological diagnoses. Among them, 30 PDACs were surgically resected and pathology obtained. Absence of PDAC was confirmed by the study coordinator’s interpretation; no progression on follow-up imaging studies, including CT and MRI for at least 6 months; or negative results on ultrasound-guided fine-needle aspiration.
Statistical analysis
To ensure adequate statistical power for detecting differences in specificity between the conventional and optimal image datasets, the required sample size was calculated using Monte Carlo simulations, factoring in a fixed number of four reviewers. First, we assumed patient-level correlations ranging from 0.01 to 0.5 and generated random numbers from a bivariate Bernoulli distribution, assuming a specificity of 80% for the conventional image dataset and 90% for the optimal image dataset. Next, we used a generalized estimating equation model with an exchangeable correlation structure at the patient level to test for differences in the specificity between the conventional and optimal image datasets. Finally, we performed 1000 iterations of the above steps and calculated the minimum sample size of patients without PDAC required to achieve 90% empirical power, which was 43 patients. The “rmvbin” function from the R package “bindata” was used to generate random numbers. Patients with PDAC were enrolled until the number of patients without PDAC reached 43, which was 67 patients. As measures of diagnostic performance, the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated for each method by all radiologists. Generalized estimating equation models were used to calculate each measure by all radiologists, experts, and trainees and to compare the conventional and optimal image datasets. If the diagnosis was exactly the same on the conventional and optimal image datasets or if either index was 100%, the results were not testable; therefore, the corresponding result was marked as “Not Calculated” (N.C.). The confidence ratings were considered ordinal categorical data, and an ordinal logistic regression model was used to compare the conventional and optimal image datasets for patients with and without PDAC, respectively. To accommodate data showing within-class correlations, the variance estimated from the ordinal logistic regression model was corrected using the Huber–White sandwich estimator.
Cohen’s kappa coefficient was used to assess the inter-rater reliability of each expert and trainee diagnosis, and Fleiss’ kappa coefficient was used to assess the inter-rater reliability among all radiologists. The inter-rater reliability between expert and trainee groups was compared using the z-test under the assumption that the kappa coefficient followed an asymptotic normal distribution.
Two-sided P values ≤ 0.05 were considered indicative of statistical significance. The statistical analyses were performed using the R software version 4.3.1 (www.r-project.org).



Comments (0)