
Remember me


This study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of the Hokkaido University and the Institutional Review Board or Ethics Committee of other participating facilities (#022-0274). According to the Ethical Guidelines for Medical Research on Human Subjects in Japan, this research does not involve intervention or use of samples obtained from the human body. The need for patient consent was waived as this was a retrospective study, and anonymity was secured. Therefore, the Institutional Review Boards or Ethics Committees of all participating facilities approved the use of the opt-out method, publishing the study on either the participating facility’s website or on a bulletin board.
Study populationThis multicenter, retrospective study involved three institutions in Japan and included patients with (1) advanced or recurrent lung cancer, (2) comorbid idiopathic IP, and (3) FDG-PET/CT performed within 3 months of chemotherapy. Exclusion criteria included no IP by central judgment, no PET/CT imaging, no history of anticancer therapy, and no history of chest or mediastinal radiation therapy. Pre-existing IP was classified as usual interstitial pneumonia (UIP), probable UIP, indeterminate for IP, and alternative diagnosis, according to the official American Thoracic Society/European Respiratory Society/Japanese Respiratory Society/Asociacion Latinoamericana del Torax (ATS/ERS/JRS/ALAT) statement (2022) [1]. Connective tissue diseases associated interstitial lung disease (CTD-ILD) is collagen disease-associated interstitial pneumonia. In this study, patients were defined as “those with a diagnosis of CTD-ILD after a visit to a collagen disease physician”, not a case of suspected collagen disease or a diagnosis of “Idiopathic Pulmonary Fibrosis Associated with Features of Autoimmunity”.
Clinical and laboratory data collected for analysisClinical and laboratory data used in this study were retrieved from patient medical records, including age, sex, height, body weight, smoking history, performance status (PS), SpO2 at rest, tumor histology, stage at diagnosis (based on the eighth edition of the TNM staging system of lung cancer), programmed cell death ligand 1 (PD-L1) status, the presence of druggable driver mutation, usage of home oxygen therapy, history of acute exacerbation of pre-existing IP, administration of steroids and anti-fibrotic agents, history of surgical resection for lung cancer, history of palliative radiation therapy, blood tests at the administration of chemotherapy and onset of AE (for albumin, C-reactive protein, hemoglobin, Krebs von den Lungen 6, lactate dehydrogenase, presence of anti-nuclear antibody), pulmonary function tests (%FVC, FVC1.0%, and % diffusing capacity for carbon monoxide (%DLco)), the latest date available to identify outcomes, survival outcomes, and cause of death in fatal cases.
FDG-PET/CT acquisition protocolImaging was conducted at each hospital using a total of 5 PET/CT systems including Biograph 64 (Siemens Healthcare GmbH, Erlangen, Germany); Discovery ST, Discovery 610, Discovery MI (GE HealthCare, Milwaukee, WI); and Gemini TF (Philips Healthcare, Cleveland, OH). As part of the clinical protocol, scans were acquired and reconstructed in accordance with institutional standards, following the guidelines established by the Japanese Society of Nuclear Medicine in 2018.
Evaluation of HRCT at baseline and the onset of AEAll diagnostic chest CTs were centrally adjudicated individually by two respiratory physicians who performed visual assessments without clinical information, and in cases where the assessments differed, a third physician made the final decision. AEs were defined as those that occurred within 6 months of the end of chemotherapy. The onset of AE was diagnosed by attending respiratory physicians according to clinical features and CT findings. Other diseases, such as infection, cancer progression, congestive heart failure, and radiation pneumonia, were carefully excluded. CT findings at the onset of AE were classified as acute interstitial pneumonia (AIP)/diffuse alveolar damage (DAD)-like pattern, hypersensitivity pneumonia (HP)-like pattern, cryptogenic organizing pneumonia (COP)-like pattern, nonspecific interstitial pneumonia (NSIP)-like pattern, and others according to the ATS/ERS international multidisciplinary classification of IP [16].
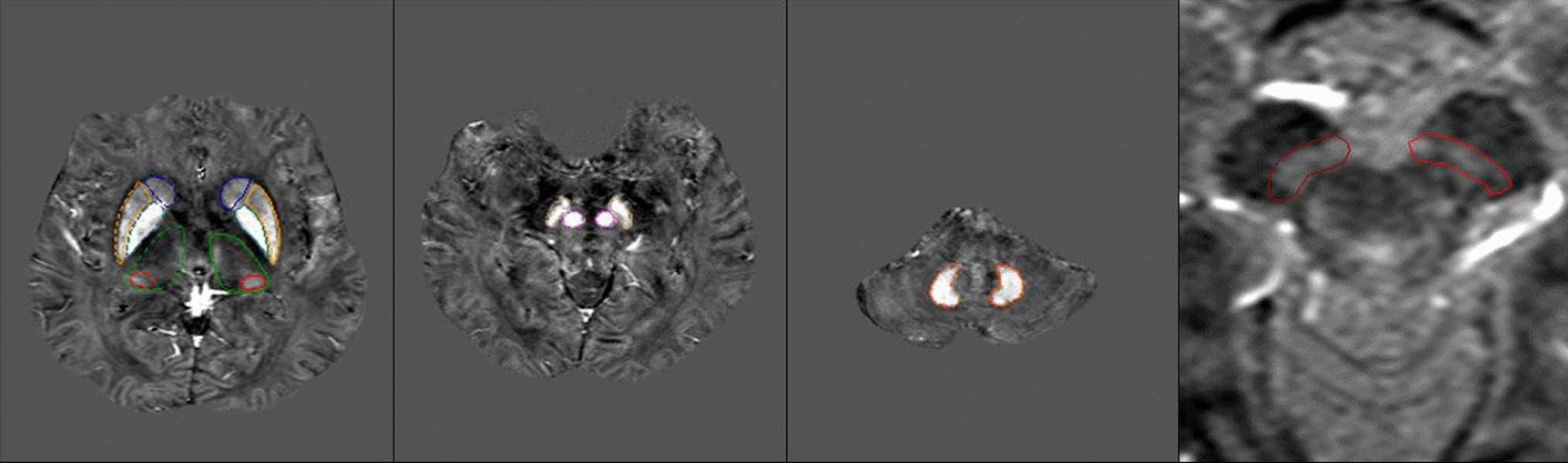
Evaluation of FDG-PET at baselineFDG-PET/CT images were interpreted independently by a board-certified radiologist and a respiratory physician. The peak standardized uptake value (SUVpeak) of each interstitial lesion, which we identified on the CT images of patients with IP, and the tumor were measured using a spherical region-of-interest with a variable diameter on PET images (Fig. 1). The value of a 1 cm3-volume spherical volume of interest (VOI) where FDG uptake centering around the hottest point in the foci was defined as the SUVpeak [17]. Technical and physiological factors may influence SUVs. Therefore, especially in a multicenter trial, it is preferred not to use absolute SUVs but residual uptake values in a tumor area normalized to an intra-image reference uptake. The target-to-blood ratio (TBR) was calculated using a spherical VOI set at 5 mm in the aorta as reference uptake, the target-to-liver ratio (TLR) set at 30 mm in the liver, and the target-to-normal ratio (TNR) set at 20 mm in the ipsilateral and contralateral normal lung in the same slice at the aortic arch and tracheal bifurcation (Fig. 2). The SUVpeak for both bilateral lung interstitial lesions were calculated from FDG-PET/CT images before chemotherapy and included those corrected by dividing by the SUVmean of references. The ipsilateral side refers to the lung with the main recurrent lesion, whereas the contralateral side refers to the other lung.
Fig. 1
FDG accumulation in the interstitial lesions. Representative cases of strong (A, B) and weak (C, D) FDG accumulation with SUVpeak values of 2.30 and 1.72, respectively, on PET-CT in the interstitial lesions
Fig. 2
Reference organs to correct for SUVpeak. A A spherical volume of interest (VOI) was set at 5 mm for the aorta, B 30 mm for the liver, and VOI of the lungs was 20 mm, and the mean values of C the aortic arch and D tracheal bifurcation of the bilateral lungs were used
In this study, FDGscore was evaluated at 20 sites to assess the extent of FDG accumulation in interstitial lesions: the anterior, middle, and posterior regions of both lungs at three anatomical levels (aortic arch, tracheal bifurcation, and maximal right atrial level), and at the diaphragmatic surface. Each site was scored on a 5-point scale: 0, no uptake; 1, uptake below the blood pool; 2, uptake above the blood pool and below the liver; 3, uptake equivalent to more than the liver; and 4, uptake markedly higher than the liver. Sites overlapping with tumors were deemed unevaluable. The total score ranged from 0 to 80 points. FDGscore was defined as the average score of the two evaluators divided by the full score, excluding the unevaluable sites. We used the FDGscore to conduct analyses comparing patients with and without AE.
Statistical analysisCategorical variables were presented as numbers (percentages) and compared using Fisher’s exact test. Non-normally distributed continuous variables were presented as median (interquartile ranges) and compared using a Mann–Whitney U test. A p value of < 0.05 was considered statistically significant. First, in order to investigate the relationship between clinical or imaging factors and FDG accumulation in interstitial lesion, we divided the patients into two groups based on the presence or absence of nominal variable factors and the median of continuous variable factors, and compared SUVpeak. Next, to investigate the association of various parameters with the risk of AE, clinical characteristics, baseline HRCT findings, FDG-PET/CT parameters, and various laboratory data were compared between patients who developed AE and those who did not. Subsequently, logistic regression analysis was performed to identify risk factors for the development of AE.
Comments (0)