Study design
This was a retrospective cohort study of patients who had a new patient visit at a single, university-affiliated fertility center between April 2020 and March 2021. All patient data was collected from the electronic medical record (EMR) with exposure status and outcomes manually validated by individual chart review. The primary exposure of this study was initial visit type (in-person versus telehealth). Patients had the autonomy to choose between telehealth with audio and visual capabilities versus an in-person office visit. The study protocol was approved by an institutional review board (Advarra IRB, Pro00027158).
Study participants
Patients who had previously created embryos or frozen oocytes at an outside clinic, planning oocyte or embryo banking for fertility preservation purposes, or individuals utilizing donor gametes or gestational carriers were excluded. The time frame of April 2020 to March 2021 was chosen due to the change in practice patterns during the COVID-19 epidemic, whereby an increased number of patients were choosing to interact with providers through telehealth. During the study period, in-person consultation continued to be offered with the same availability as prior to the COVID-19 epidemic, allowing an objective comparison between initial patient visit types.
Data collection
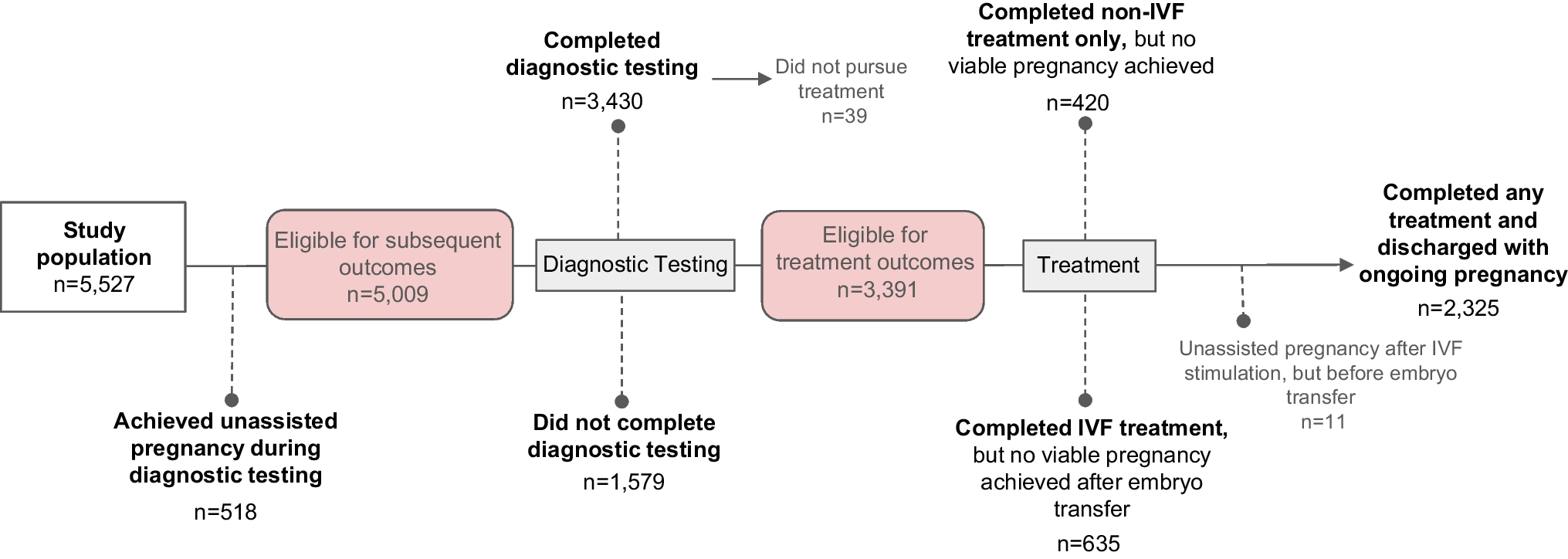
The primary outcome of this study was ongoing pregnancy as a result of fertility treatment with subsequent discharge to obstetrical care at approximately 8 weeks of gestation. Secondary outcomes included the highest level of patient engagement achieved, defined as the furthest stage in clinical assessment and treatment of infertility, if the patient did not achieve the primary outcome. Levels of patient engagement were detailed as follows: achieved unassisted pregnancy during diagnostic testing; did not complete diagnostic testing; completed diagnostic testing but did not pursue treatment; completed diagnostic testing and non-in vitro fertilization (IVF) treatment (ovulation induction with fertility medication (OI) with intrauterine insemination (IUI), OI with timed intercourse (TIC), or IUI alone) but did not achieve a viable pregnancy; completed diagnostic testing and IVF treatment but did not achieve a viable pregnancy. All patients were required to complete diagnostic testing prior to pursuing treatment. If appropriate, patients first utilized non-IVF methods to conceive, followed by IVF if pregnancy was not achieved as part of shared decision-making with their individual provider. Patients who achieved an ongoing pregnancy as a result of non-IVF treatment did not utilize IVF during the study period; patients who achieved an ongoing pregnancy as a result of IVF treatment may or may not have previously utilized non-IVF methods but were ultimately not able to achieve pregnancy with those treatments.
Other important covariates collected for analysis included key patient characteristics such as age at first visit, body mass index (BMI, kg/m2), primary infertility diagnosis, day 3 follicle-stimulating hormone (FSH, IU/L), anti-Müllerian hormone (AMH, ng/mL), antral follicle count (AFC), partner status (yes/no), same-sex couple status (yes/no), time of patient follow-up from initial consultation to final pregnancy outcome data extraction (days), and type of fertility treatment (non-IVF versus IVF). Patient age, BMI, FSH, AMH, and AFC were explored as both continuous and categorical variables for descriptive purposes, but continuous categorization was utilized for model building.
Statistical analysis
This study examined the association between initial fertility visit type and ongoing pregnancy as a result of fertility treatment. Baseline characteristics for those who utilized telehealth versus an in-person visit for initial fertility consultation were compared using Pearson’s chi-square test for categorical variables and the two-sample t-test or Wilcoxon rank-sum test for continuous variables that were normally or not normally distributed, respectively. For the primary analysis, multivariable logistic regression was used to identify associations of visit type with discharge with an ongoing pregnancy after adjusting for possible confounders in the entire study population. To account for expected differences in rates of pregnancy by treatment type (non-IVF versus IVF), the fully adjusted model included only those who had utilized fertility treatment to achieve pregnancy to allow stratification for infertility treatment type (non-IVF versus IVF).
Potential confounders were selected a priori based on known biologic plausibility and included maternal age (years), body mass index (BMI, kg/m2), primary infertility diagnosis, anti-Müllerian hormone (AMH, ng/mL), partner status (yes/no), same sex couple status (yes/no), and time from initial visit (days). For the primary outcome of ongoing pregnancy as a result of fertility treatment, partner status and same sex status were not included in the model to optimize parsimony. Day three follicle-stimulating hormone (FSH) and antral follicle count (AFC) were also not included due to collinearity with AMH as well as being duplicative measures of ovarian reserve and predicted response to fertility treatment. Because unassisted pregnancy has not been shown to be associated with AMH, this variable was not included in the analysis for this outcome. Additionally, if a patient had an unassisted pregnancy at any time, we did not include these patients in subsequent analyses of stages of patient engagement, as they no longer needed to proceed with care and, therefore, were not able to have these other outcomes. Depending on the model and after excluding patients who no longer could have specific engagement outcomes (i.e., those with unassisted pregnancies), missing covariate values ranged from 7.6 to 12.3%. Given this small range of missingness and our large sample size, we utilized complete case analysis.
All statistical analyses were performed in STATA software version 17.0 (College Station, Texas). A p-value of < 0.05 was considered to be statistically significant.


Comments (0)