Main findings
The present study reports a relatively high prevalence of vaginal dysbiosis in IVF patients defined either as AVM (34%) or CST-IV (48%). We corroborate the findings of previous studies in non-IVF patients that also in IVF patients vaginal dysbiosis is associated with higher BMI, alcohol consumption, and smoking. Fishy odor was reported relatively rarely but was significantly more common in patients with AVM or CST IV when compared to patients not reporting this symptom. Likewise, tubal factor infertility was significantly associated with prevalent AVM or CST IV-A and IV-B. AVM was previously defined as a means to have a reliable and fast turn-around method to identify IVF patients with vaginal dysbiosis associated with a poor reproductive outcome [9]. We confirm previous results that the AVM diagnosis correlates well with BV-type microbiota CST IV-A and IV-B; albeit, more rarely, AVM can also be found outside of these CSTs. As could be expected, the dominating CST among the non-AVM positive patients was CST I (41%). In contrast, women with AVM predominantly had CST-IV-B dysbiosis (56%) followed by CST III (12%), CST IV-A (10%) and CST IV-C (11%).
Despite no guidelines recommending the use of soaps for intimate washing, we report that 63% of the patients used soaps as part of their intimate washing regimen. In a small sub-cohort undergoing interview, IVF patients reported that they used the particular washing regimen daily in order to feel clean. Moreover, even though clinical guidelines recommend against vaginal douching, this was done by 19% of the patients, and douching was significantly associated with vaginal dysbiosis, as previously reported for non-IVF patients [17] Finally, the use of low pH soap was significantly more common in IVF patients with vaginal dysbiosis, whereas the use of a menstrual cup was reported significantly more often by patients not having AVM.
Strengths and limitations
The present study is a large cross-sectional study including 1533 IVF patients screened for AVM prior to an RCT. Thus, the present study by design cannot infer causal inference but only report associations between vaginal dysbiosis and the variables described. To our knowledge, this is the largest study in IVF patients to describe such associations, including a description of intimate health habits. The study population consisted of primarily Caucasian IVF patients, limiting the generalizability to other populations.
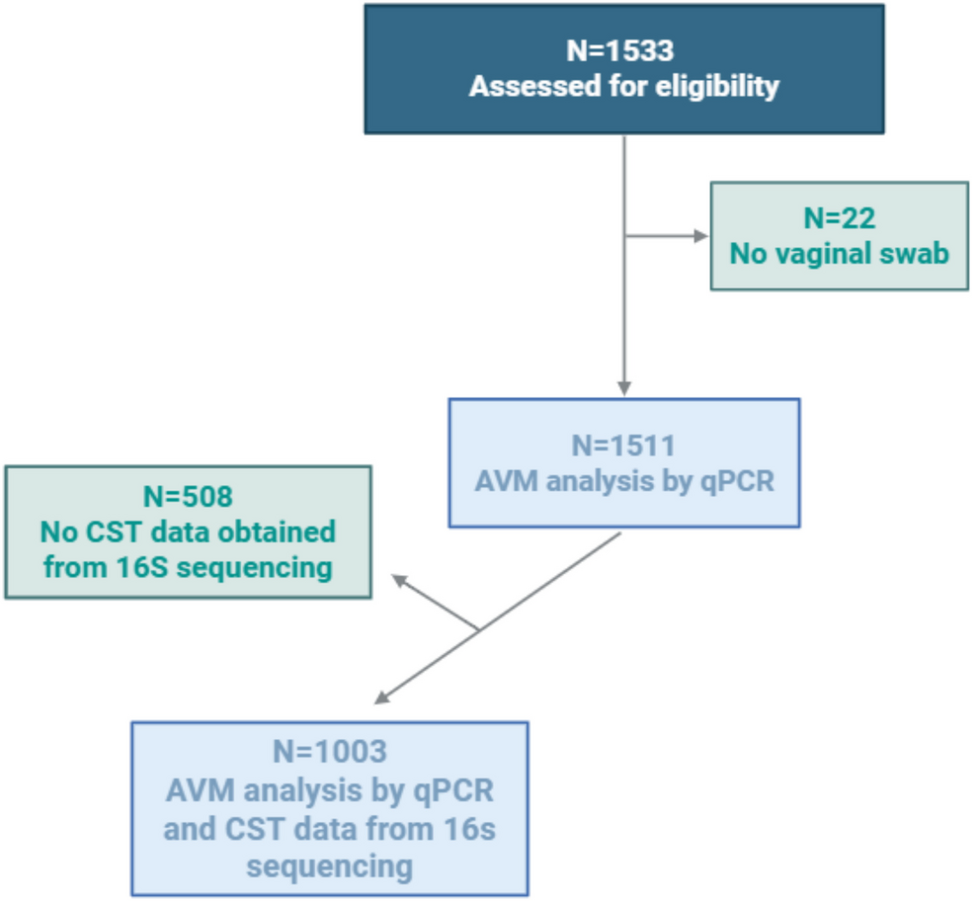
In March 2019 questions on the use of menstrual products were added, with a total of 1153 women completing the questionnaire (Fig. 1). This should not give cause for selection bias since the IVF patients were included sequentially by the same inclusion criteria, only at a later point in time. We cannot exclude a recall bias of the self-reported gynecological symptoms. Vaginal microbiota was investigated by means of both a qPCR method and a 16S rRNA gene sequencing-based method. Longitudinal studies have shown that the vaginal microbiota varies over the menstrual cycle [18]. A limitation of our study is that patients were screened at different days in the menstrual cycle and only on one day each.
Interpretation
In a recent meta-analysis of observational studies, the prevalence of vaginal dysbiosis was 19% (1271/6835, 95% CI 18–20%) [19]. In the present study, we report a significantly higher prevalence of vaginal dysbiosis defined by either AVM (34%) or CST-IV (48%). The AVM prevalence reported herein is relatively similar to our previous pilot study in which we reported an AVM prevalence of 28% (N = 36/130) [9]. However, in that same cohort, the CST IV prevalence was only 17% (N = 20/120), which is significantly different in the present larger cohort. It is not straightforward to explain this difference, although we found that patients with CST IV-C seem to be highly correlated with recent menstruation whereas AVM, CST IV-A, and IV-B do not. The present larger study may have sampled more women within seven days of menstruation compared to our pilot study, which could in part explain a difference in CST IV prevalence. Importantly, it is reported herein that an AVM diagnosis, which was the primary diagnostic marker for intervention in a subsequent RCT, was not related to recent menstruation, which is in line with the basic idea behind the qPCR method, targeting a high quantity of BV-type bacteria prior to the IVF embryo transfer procedure.
Lifestyle and hygiene habits may affect the vaginal microbiota; in particular, smoking [20, 21], increased BMI [21], and low dietary fiber intake [22] are all associated with vaginal dysbiosis. Herein, we confirm these findings; albeit, we do not have information on dietary habits, which could be interesting to investigate further. As the normal vaginal microbiota acts as a defense system against ascending infections, a serious implication of vaginal dysbiosis may be an increased risk of acquiring other genital tract infections such as Chlamydia, Gonorrhea, HSV, HPV [23], and possibly also Mycoplasma genitalium. Consequently, these infections may lead to complications such as pelvic inflammatory disease and tubal factor infertility (TFI). In the present study, IVF patients who previously had a chlamydia infection were significantly more likely to have AVM. Moreover, and perhaps consequently, TFI was also significantly associated with a higher prevalence of AVM and CST IV-A + B. It is interesting to speculate if the higher AVM prevalence in women with TFI or previous chlamydia is the result or the cause. If a treated infection can lead to persistent changes in the microbiota, this may justify studies on the mechanism behind this.
In line with the present results, douching has repeatedly been associated with vaginal dysbiosis [17, 21]. At the clinic, in line with international recommendations, we recommend that douching should not be practiced. It has been a generally held belief that douching is not used among women in Denmark today. Thus, we were surprised to find that 19% of IVF patients practice vaginal douching. It appears that there is an incentive to achieve a feeling of cleanliness, as reflected in the answers from the small subpopulation interview. Thus controversial, as one could argue this practice may result in the exact opposite of what is intended by these women: a disruption in dominance of Lactobacillus spp. and a higher prevalence of vaginal dysbiosis. We do not know how common douching is among Danish women in general, compared to this group of IVF patients. It is interesting to speculate whether this group of women is more motivated to feel clean due to a fertility desire while undergoing fertility treatment with frequent gynecologic exams and procedures.
The use of intimate soap was significantly associated with AVM/CST IV-A + -B in IVF patients. Despite low pH, intimate soap might disrupt the balance of the vaginal microbiota, albeit interpretation must be done with caution as the present study cannot distinguish if the use of a product is due to symptoms such as smell, itch, or change in discharge—or if the product induces dysbiosis. Perhaps the use of soaps is higher due to an attempt to alleviate symptoms of vaginal dysbiosis.
In the entire study population, 37% of the women used intimate soap, but of women who had reported fishy odor, a total of 55% used intimate soap. Considering self-reported vaginal gynecological symptoms, only vaginal fishy odor symptoms were significantly more common among patients with AVM compared to patients without AVM. Moreover, IVF doctors did not document significantly more BV symptoms in the AVM group (data not shown).
Conflicting results have been reported on the use of menstrual products. Our results showed no significant correlation between vaginal microbiota and the use of tampons or pads. In contrast, IVF patients using a menstrual cup were significantly less likely to have AVM. In a recent RCT, the use of a menstrual cup in Kenyan women is shown to significantly reduce BV and improve relative abundance of L. crispatus [24]. Future studies may enable optimized evidence-based recommendations on intimate health hygiene health, which is evidently needed as women prioritize the importance of feeling clean.


Comments (0)