
Remember me
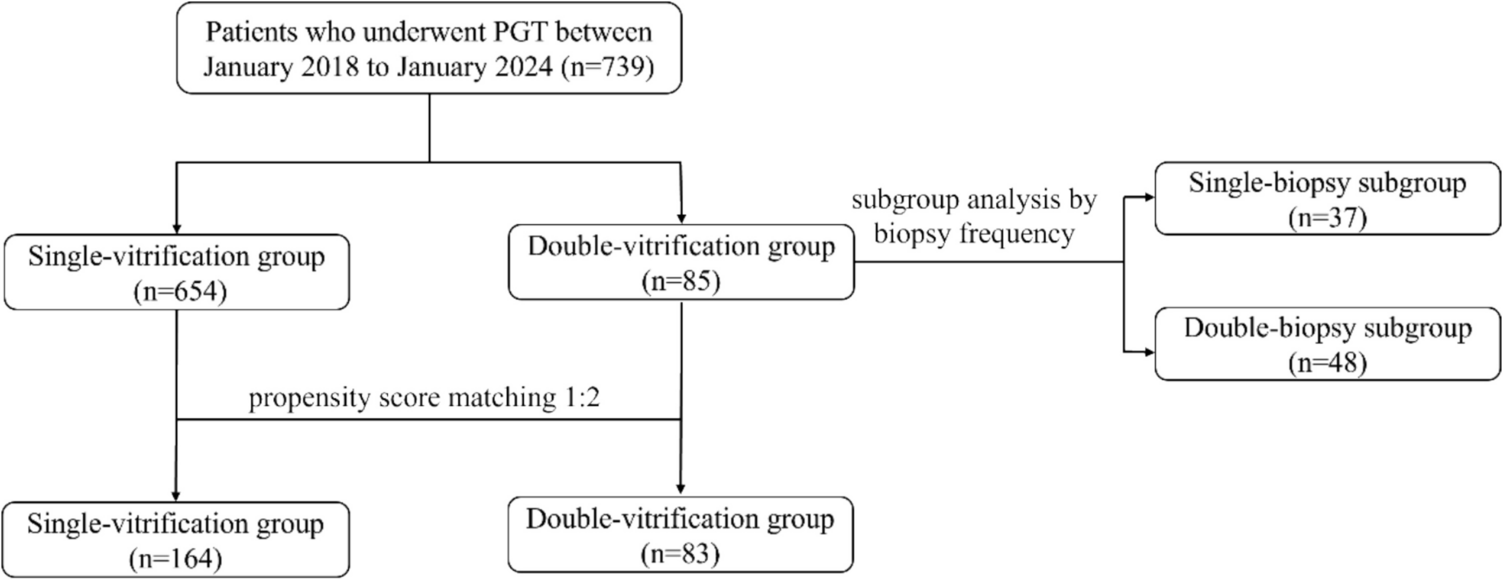

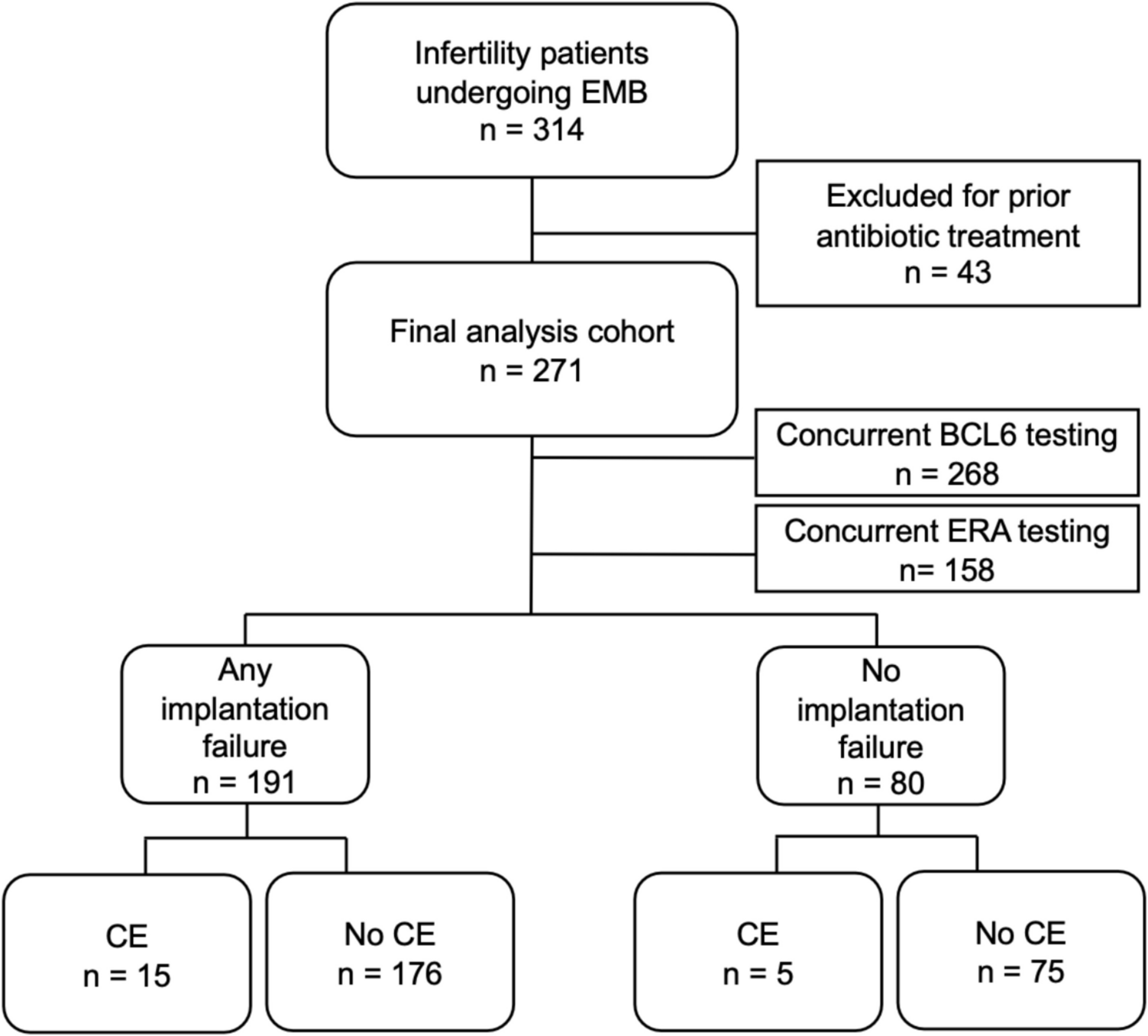
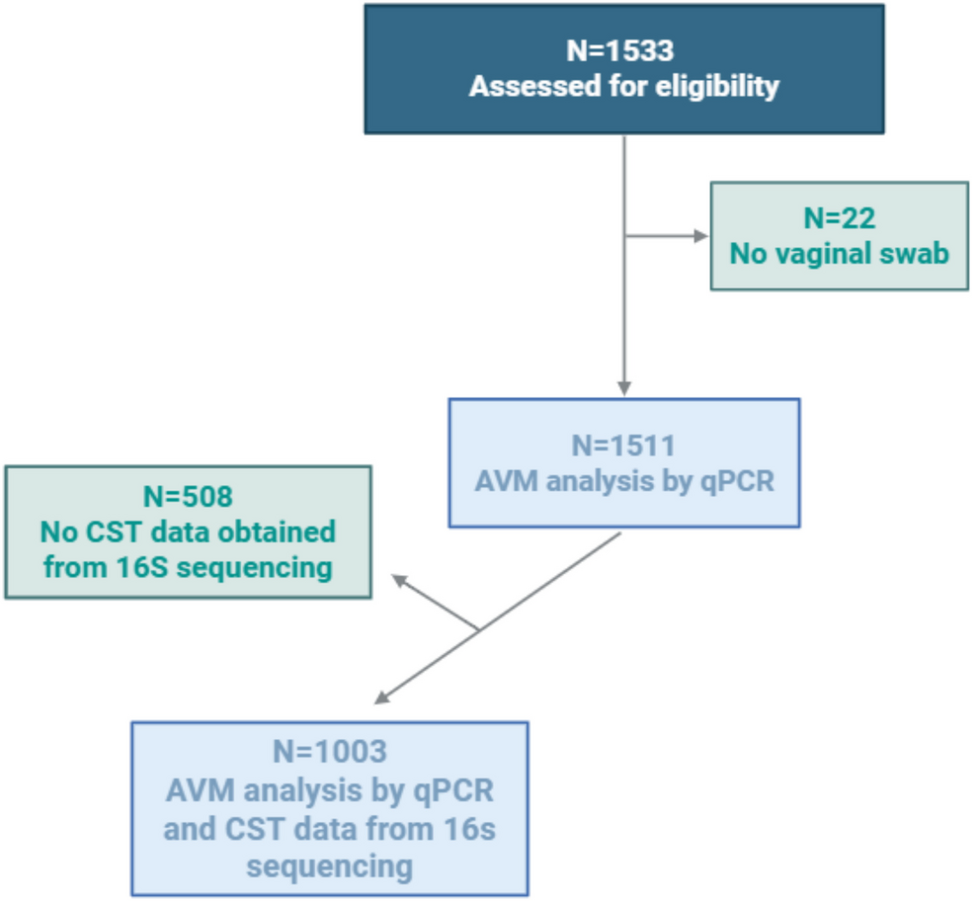
This study involved the collection of clinical data from patients who underwent PGT-A at the Center for Reproductive Medicine of the General Hospital of the Northern Theater of Operations from January 2018 to August 2024. The patients were selected based on the indications of advanced maternal age (AMA), recurrent spontaneous abortion (RSA), or recurrent implantation failure (RIF). A retrospective analysis was conducted, and the flowchart of this study is shown in Fig. 1.
Fig. 1
Flowchart of the study on the correlation between AMH levels and embryonic aneuploidy rate
Inclusion criteria: Patients fulfilling any of the above criteria were qualified for inclusion. (1) AMA (female age ≥ 38 years old); (2) RSA (defined as ≥ 2 spontaneous abortions); (3) RIF (defined as ≥ 3 transfers or a cumulative total of ≥ 4–6 high-quality embryos or ≥ 3 high-scoring blastocysts still not implanted).
Exclusion criteria: (1) chromosomal abnormality in either spouse; (2) history of ovarian endometriosis or ovarian surgeries; (3) endocrine or autoimmune diseases (e.g., diabetes mellitus and systemic lupus erythematosus); (4) use of egg donation; (5) severe teratospermia in the male partner (defined as having <1% normal sperm morphology); (6) incomplete core data in the medical record.
Ovulation regimenDepending on the woman’s age and ovarian reserve, an appropriate ovarian stimulation regimen is used for ovulation or natural cycle egg retrieval. Ovulation induction regimens include agonist regimens [gonadotropin-releasing hormone (GnRH) agonist long regimen, GnRH agonist extra-long regimen, GnRH agonist short regimen], GnRH antagonist regimens, and other regimens. Other regimens included the use of recombinant follicle-stimulating hormone (recombinant follicle-stimulating hormone, r-FSH, Jinseheng, Changchun Jinsai Pharmaceutical Co. Ltd; gonadotropin, Merck Serono, USA)/urine-derived human menopausal gonadotropin (HMG, Lebold, Lizhu Pharmaceutical Factory, Zhuhai Lizhu Group) direct stimulation, microstimulation, luteal phase ovulation, and natural cycle egg retrieval regimens. The Gn initiation dose was determined based on the woman’s age, AMH, basal antral follicle count (bAFC), body mass index (BMI), and ovarian response in previous cycles. When at least one follicle was ≥ 18 mm in diameter, follicle maturation was induced by injection of 250 µg of recombinant human chorionic gonadotropin (r-hCG, Azer, Merck Serono Ltd., Switzerland). Egg retrieval was performed 24–36 h after r-hCG injection.
Culture of embryosMature oocytes at the metaphase II (MII) phase were fertilized in vitro using intracytoplasmic single sperm microinjection technique. The fertilized oocytes were initially cultured in oviduct fluid culture (ART-1026) for 60–72 h, followed by transfer to blastocyst oviduct fluid culture (ART-1029) for an additional 48–72 h.
Blastocyst biopsyA morphologic evaluation system for oocytes and early embryos was used for embryo culture. Embryos with 6–10 cleavage cells on day 3, classified as grade 1 or 2, were considered high-quality embryos. Blastocysts were assessed according to the Gardner scoring criteria, and trophoblast cell biopsies were performed on blastocysts with a score of ≥ 4 BB. A laser was used to create a hole of approximately 50 µm in diameter at the contralateral position of the inner cell mass of the blastocyst to be biopsied. Six to eight trophoblast cells were aspirated from the biopsy pins into the notch and detached from the blastocysts using both laser and mechanical methods. The biopsied cells were transferred to PCR tubes containing phosphate-buffered saline and stored in an ice box for further examination. PGT-A was performed by whole genome SurePlex amplification of the biopsied trophoblast cells. Amplification and library construction were conducted using the PGT-A kit (Beijing Zhongyi Kangwei Medical Equipment Co., Ltd.). Sequencing was performed using the Illumina sequencing platform MiSeqDx sequencer, and the sequencing data were analyzed for chromosome copy number using the Embryonic Chromosome Alloploidy Analysis System software (Beijing Zhongyi Kangwei Medical Equipment Co., Ltd.). The analysis process involved quality control of the sequencing data, followed by comparison to the human reference genome (GRCH37/hg19). The whole reference genome was divided into multiple windows, and the number of reads in each window was calculated. Copy number analysis was performed by bioinformatics algorithm through the data correction, combined with the reference range established by the reference dataset. The resolution of the detection was 4 Mb. When the proportion of 4 Mb and above copy number variation and chromosome abnormality was greater than 80%, the blastocyst was judged to be aneuploid. If the proportion of abnormality was between 30 and 80%, the blastocyst was recognized as a chimeric blastocyst.
Frozen embryo transfer (FET) protocolAfter obtaining a euploid embryo, the endometrial preparation protocol prior to FET is selected based on the patient’s age, endometrial thickness, and the presence or absence of comorbid adenomyosis. The endometrial preparation regimen mainly consists of natural cycle regimen, estrogen replacement cycle regimen, GnRH-a down regulation plus estrogen replacement cycle regimen, and ovulation induction cycle regimen. The endometrial thickness, estrogen, and progesterone levels of all transfer programs must meet the criteria for transfer before the frozen-thawed embryo transfer procedure is performed. All types of transfer programs require pharmacological luteal support, the dose of which is adjusted according to the levels of estrogen and progesterone, and the luteal support is continued after the transfer. If pregnancy is confirmed, the original dosage will be maintained until the 8th week of pregnancy, and then the dosage will be gradually reduced until the 12th week of pregnancy.
Clinical indicatorsThe following clinical indicators were recorded: female age, male age, BMI, years of infertility, number of cycles, basic follicle-stimulating hormone (bFSH), basic luteinizing hormone (bLH), basic estradiol (bE2), AMH, bAFC, and total gonadotropin (Gn) dose.
Measurement of indicatorsAMH levels were measured using venous blood collected at any point during the menstrual cycle in the year prior to ovulation induction. bFSH, bLH, bE2 were measured from venous blood collected on days 2–5 of the natural menstrual cycle. bAFC was determined by transvaginal ultrasonography on days 2–5 of the menstrual cycle, with follicles ranging in size from 2 to 8 mm considered antral follicles, and the total count of these follicles was recorded. BMI was calculated as body weight (kg) divided by height (m)2. The euploidy rate was calculated by dividing the number of euploid blastocysts by the number of biopsied blastocysts, multiplied by 100%. Similarly, the aneuploidy rate was calculated by dividing the number of aneuploid blastocysts by the number of biopsied blastocysts, multiplied by 100%. The mosaic rate was calculated by dividing the number of chimeric blastocysts by the number of biopsied blastocysts, multiplied by 100%. The fertilization rate was calculated by dividing the number of normally fertilized oocytes by the total number of eggs obtained, multiplied by 100%. The day 3 high-quality embryo rate was calculated by dividing the number of high-quality embryos on day 3 by the number of embryos with two pronuclei (2PN), multiplied by 100%. The blastocyst formation rate was calculated by dividing the number of blastocysts formed on day 5 or day 6 by the number of embryos with 2PN, multiplied by 100%. The diagnosis of a live birth is made when the gestational age of the pregnancy is 28 weeks or more, the fetal weight is greater than 1000 g, and the fetus exhibits vital signs following delivery.
Statistical analysisPatients who met the criteria were divided equally into three groups based on their AMH values by percentile, using the 25th percentile and 75th percentile as cutoffs. Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed variables were expressed as mean ± standard deviation (SD), while skewed continuous variables were expressed as median and interquartile range (IQR). Categorical variables were expressed as frequencies and percentages (%). To assess differences between groups, the chi-square test was used for categorical variables, ANOVA for normally distributed continuous variables, and the Kruskal–Wallis test for skewed continuous variables. Potential confounders were identified based on the following criteria: a P-value < 0.1 in univariate analysis or a change of more than 10% in the effect size in covariate screening. Variables with covariates related to AMH were excluded from multifactor regression analysis. Univariate regression analyses were performed on the remaining variables to identify potential factors influencing the embryonic aneuploidy rate. Multifactorial logistic regression analysis was performed with aneuploidy rate as the dependent variable (with a rate ≥ 0.5 defined as a positive event) and AMH as the independent variable. Variables with P-values < 0.1 and changes in effect size greater than 10% during covariate screening were included in the multifactorial model using forward selection. Subsequently, variables with P-values < 0.05 from the multifactor logistic regression were included in the regression model for RCS, with nodes at specific percentiles (5th, 35th, 65th, and 95th). The results were expressed using odds ratios (OR) and their 95% confidence intervals (CI). A two-stage logistic regression model was used to analyze the threshold between AMH levels and aneuploidy rates. Inflection points were identified using likelihood ratio tests and bootstrap resampling methods. To assess the stability of the relationship between AMH and embryonic aneuploidy across populations, stratification analyses were performed based on the following subgroup variables: female age (< 35 years, 35–37 years, > 37 years), BMI (15–24 kg/m2, > 24 kg/m2), infertility type (primary infertility, secondary infertility), and number of years of infertility (< 2 years, 2–4 years, > 4 years), PGT-A factors (AMA, RSA, RIF); heterogeneity between subgroups was assessed by multivariate logistic regression, and interactions between subgroups and AMH were assessed using the likelihood ratio test. Univariate and multivariate logistic regression analyses of live birth outcomes were performed using the same methods previously described. A subject operating characteristic (ROC) curve was established to explore the predictive ability of AMH values for live birth in euploid embryo transfer. Missing data were addressed using multiple interpolation methods, following the approach outlined by Van Buuren and Groothuis-Oudshoorn (2011). All analyses were performed using R statistical software (http://www.R- project.org, the R Foundation) and the Free Statistics analysis platform, and differences were judged to be statistically significant at P < 0.05 (two-tailed).
Comments (0)