SUV measurements are not yet a standard part of routine [18F]FDG PET/CT interpretation in paediatric oncology, primarily being employed in research settings. However, metrics such as metabolic tumour volume (MTV) and total lesion glycolysis (TLG), along with SUV measurements, are increasingly utilized in research protocols to evaluate tumour burden and monitor treatment response. In paediatric oncology, understanding weight dependency is particularly relevant due to the significant variability in body composition among children of different ages and developmental stages.
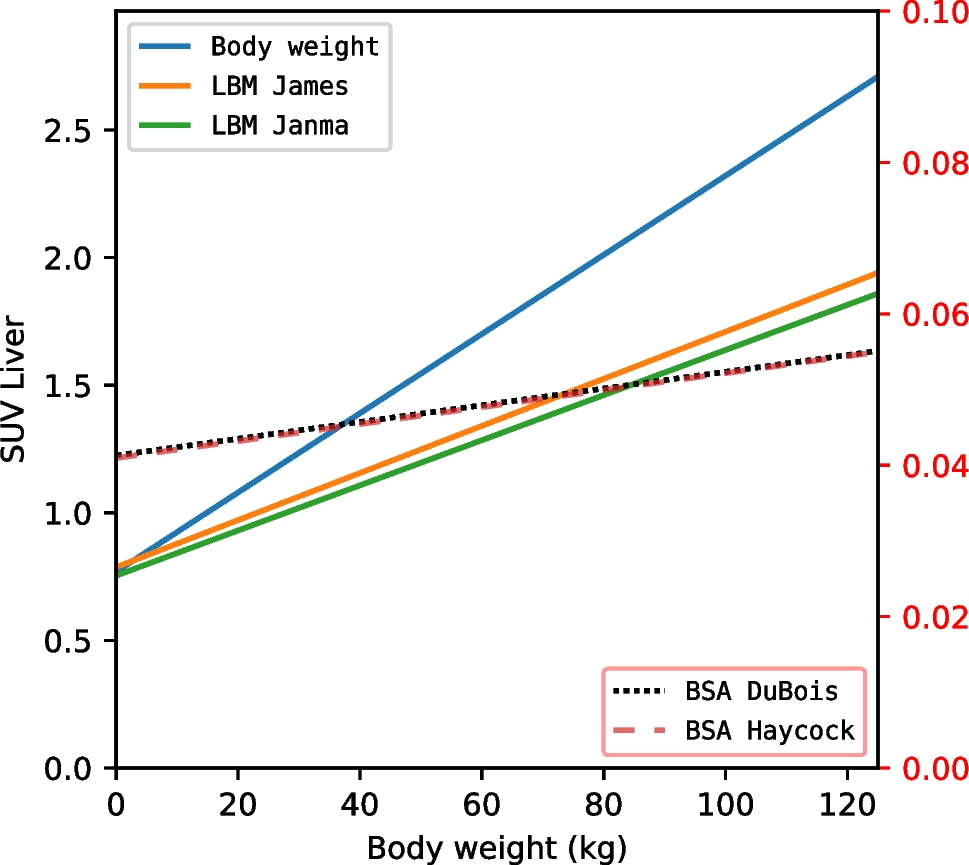
This study aimed to compare different SUV formulations in paediatric oncology patients and assess their dependency on body weight. In a large dataset of 461 [18F]FDG PET/CT scans, our findings confirm that SUVBW exhibits the highest dependency on body weight compared to the SUVLBM formulations (SUVLBMJames and SUVLBMJanma) and the SUVBSA formulations (SUVBSADuBois and SUVBSAHaycock). These results are consistent with previous studies involving adults and a small paediatric population, which have demonstrated that SUVLBM and SUVBSA adjustments reduce weight dependency in SUV measurements [1, 2, 7, 17].
Use of different SUV metrics has been extensively validated against full kinetic analysis in adult populations, such as the studies by Hoekstra et al. and Freedman et al. [18, 19]. These studies highlighted the importance of aligning SUV calculations with physiological considerations to improve accuracy and reduce variability. Although these validations were performed in adults rather than children, they provide important context for the current findings, as we observe similar patterns of reduced weight dependency with SUVLBM and SUVBSA formulations. Our findings align with these earlier observations, further supporting the broader utility of SUVLBM as a robust metric in [18F]FDG PET imaging.
Among the different SUV formulations studied, SUVBSADuBois and SUVBSAHaycock showed the lowest dependency on body weight. For example, based on our dataset, the SUVBW in the liver varied significantly between a child weighing 10 kg and one weighing 40 kg, with SUVs of 0.97 and 1.57, respectively, a difference by a factor of 1.62. In contrast, SUVBSAHaycock varied only slightly, by a factor of 1.08, between the same two children, with SUVs of 0.04112 and 0.04448, respectively. These findings suggest that SUVBSA formulations may provide more reliable measurements in paediatric patients, particularly when body weight varies considerably.
A major strength of this study is the inclusion of a large cohort of 461 paediatric patients, all of whom were scanned on the same [18F]FDG PET/CT system. This consistency, combined with the wide range of patient ages, enhances the generalisability of our findings to the broader paediatric population.
However, several limitations should be acknowledged. First, the restriction to the first [18F]FDG PET/CT scan during the study period precluded an analysis of how SUV measurements change over time in individual patients. This could be an important consideration in assessing treatment response. Second, since all SUV formulations incorporate body weight to some degree, the correlation with body weight was never fully eliminated, limiting the independence of these correlations. Third, we did not account for the potential influence of factors like glucose and tumour load. It is known that these factors can influence SUV as they influence the distribution of [18F]FDG throughout the body. Last, we did not account for the potential influence of chemotherapy administered to an unknown number of patients before the [18F]FDG PET/CT scan, which may have impacted SUV measurements, particularly in the liver. However, we mitigated this limitation by also measuring SUV in the blood pool, where chemotherapy has minimal influence, to serve as a control and ensure robustness of our findings.
Our findings have important clinical implications for paediatric [18F]FDG PET/CT imaging. Given the strong dependency of SUVBW on body weight and its tendency to inflate values in heavier patients, this formulation should be avoided in routine clinical practice. Both SUVLBM and SUVBSA formulations offer lower dependency on body weight and thus provide more consistent assessments across different patient groups. While the equations for LBM and BSA are empirically derived and widely validated for adults, their applicability in paediatric patients should be carefully considered. The BSAHaycock formulation, specifically developed and validated for children, is particularly suited for paediatric applications and has also been widely adopted in pharmacokinetics due to its geometric basis and broad applicability across ages [6]. Nonetheless, these equations may not accurately represent body composition in extreme cases, such as top athletes or patients with atypical body proportions, which could limit their generalizability in certain context. Interestingly, BSA appears to perform better than LBM as a normalisation factor in this paediatric population, likely due to differences in [18F]FDG clearance mechanisms between children and adults. In adults, only up to 10% of [18F]FDG is excreted via urine within 60 min post-injection, whereas in children, kidney clearance and the correlation of BSA with cardiac output and blood volume may play a larger role in [18F]FDG distribution. Additionally, the percentage of body fat in children fluctuates considerably, reaching up to 25% during the first year of life, which may limit the accuracy of LBM as a surrogate. While LBM is a good indicator of liver metabolism, its practical applicability appears less robust in children compared to BSA.
Normalisation metrics like body weight, LBM, and BSA aim to approximate the bioavailability of [18F]FDG from blood to tissues by accounting for factors such as blood volume and clearance mechanisms. Body weight normalisation is simple but fails to consider body composition variability. LBM improves upon this by excluding adipose tissue, but fluctuating fat percentages in children limit its reliability. BSA, with its strong correlation to cardiac output and blood volume, provides a better surrogate for [18F]FDG bioavailability in paediatric patients [20, 21].
It is also worth noting that SUVBSA is not unitless, as BSA is expressed in m2. This contrasts with the SUVLBM and SUVBW formulations, which can be converted to a volumetric unit by dividing by tissue density. Consequently, SUVBSA values are generally lower, complicating direct comparisons with SUVLBM and SUVBW.
Furthermore, from a practical standpoint, it would be prudent to adhere to the PERCIST (PET Response Criteria in Solid Tumours) guidelines, which recommend the utilisation of SUVLBM for the assessment of both adult and paediatric patients [22], and based on our findings, SUVLBMJames may be a particularly favourable formulation. It’s worth noting that both SUVLBMJames and SUVLBMJanma have gender specific formulations (Table 1). Unlike other formulations, SUVLBMJames did not exhibit significant differences between male and female patients, suggesting it to be a more gender-neutral option for clinical use. This is an important consideration for ensuring consistent and unbiased SUV measurements in paediatric populations.
Looking forward, advancements in imaging technology could further improve the accuracy of SUV measurements in paediatric patients. Dual-energy CT or machine learning-based body composition analysis offers the potential to provide more accurate estimates of lean body mass and body composition [23, 24]. These technologies could support better quantification of [18F]FDG uptake by providing more individualised adjustments to SUV calculations, minimising the dependency on crude body weight measures and potentially leading to even more accurate and reliable assessments of metabolic activity.




Comments (0)