
Remember me



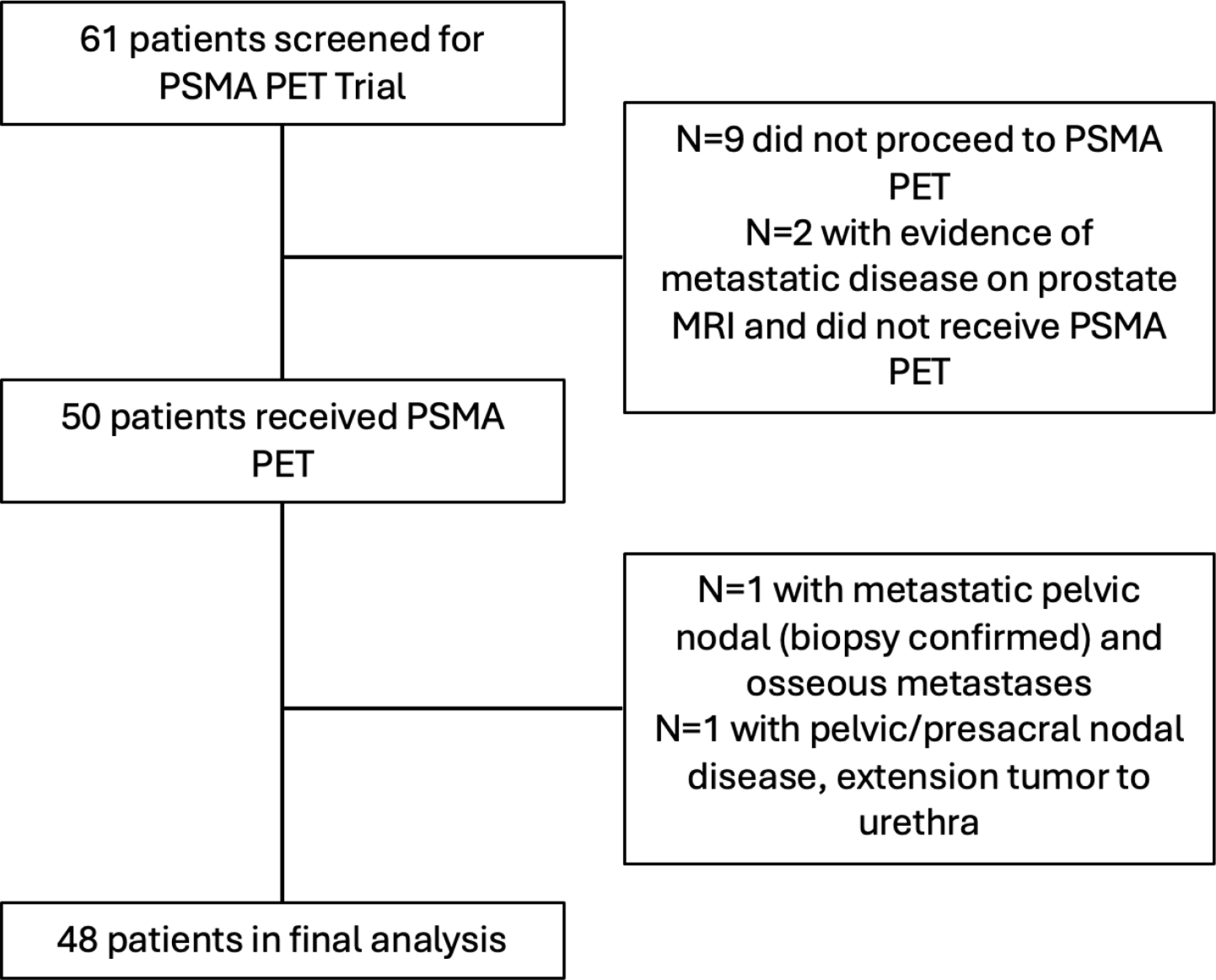
The literature search yielded 140 results. After screening titles and abstracts and applying inclusion and exclusion criteria, we selected 25 papers. The principal reasons for exclusion were as follows: the presence of a heterogeneous cohorts/mCRPC scenario, and duplicate results. A flowchart summarizing the selection process is shown in Fig. 2.
Fig. 2
Overview of the studies selection process
NeoadjuvantIn the neoadjuvant setting, Golan et al. assessed the safety and early outcome of 2–3 cycles of 7.4 GBq of [177Lu]Lu-PSMA-I&T at 2 weeks intervals before radical prostatectomy (RPE, 4 weeks after the last RLT) in 14 high-risk localized PCa with high PSMA uptake at [68Ga]Ga-PSMA-I&T PET/computed tomography (CT). The authors registered a PSA median reduction of 17% and 34% after 2 and 3 [177Lu]Lu-PSMA-I&T doses, respectively. They also observed ISUP downgrading in three patients (23%), without affecting continence recovery [23].
More recently, in the LuTectomy study, Eapen et al. investigated the dosimetry, safety, and efficacy of neoadjuvant [177Lu]Lu-PSMA-617 in 20 men with high-risk localized PCa with high-tumor uptake at [68Ga]Ga-PSMA-11 PET/CT before RPE. Study participants received one (10/20) or two cycles (6 weeks interval) of 5 GBq of [177Lu]Lu-PSMA-617, 6 weeks before RPE. After cycle one, the median highest tumor radiation absorbed dose for all lesions was 35.5 Gy (19.6 Gy to the prostate), and five study participants received radiation to lymph nodes. 9/20 (45%) patients achieved > 50% PSA decline without any G3 or higher toxicities. Interestingly, one patient had minimal residual disease on final histology, and no patients achieved a complete pathological response [24].
The NEPI trial is a single-center (Germany) randomized phase I/II study (not yet recruiting) that aims to explore neoadjuvant [177Lu]Lu-PSMA-617 with or without Ipilimumab in 58 high-risk PCa candidates for RPE (tissue specimen must be available), at maximum oligometastatic on PSMA PET with prostatic SUVmax > 12 (M1 patients at CI will be excluded). The study will start with a safety cohort assessing [177Lu]Lu-PSMA-617 dose including 6 to 12 patients (phase I); then, 46 study participants will be randomized (1:1) to receive 2 cycles of 7.4 GBq [177Lu]Lu-PSMA-617 (at 6 weeks interval) with or without 4 cycles of concomitant Ipilimumab 3 mg/kg every 3 weeks before RPE (day 1 RLT, day 3 Ipilimumab); ADT will be applied to all patients during the neoadjuvant treatment phase. The primary endpoints will be the feasibility of performing prostatectomy on time and the pathological complete response; the estimated study completion is September 2028 (NCT06388369).
The randomized, recruiting, phase I/II Nautilius is a single-center (US) trial evaluating 2 cycles of [177Lu]Lu-rhPSMA-10.1 with and without Degarelix (ADT) in 36 high-risk, localized and locoregional (M1 on PSMA PET are allowed) PSMA PET-positive (prostatic SUVmax > 8) PCa, candidate for RPE. Included participants must be M0 on CI and must have a minimum prostatic volume of 1.5 cm3 on MRI. The primary endpoints will be the safety, and the RLT efficacy based on radiation dose to the tumor and PSA assessment; the estimated study completion is June 2026 (NCT06066437).
Finally, NCT06259123 is a single-center phase II trial (Austria), recruiting 10 oligometastatic PCa planned for RPE diagnosed by [68Ga]Ga-PSMA-11 PET (M1a, and/or M1b with ≤ 5 bone metastases, and/or M1c with ≤ 3 lung metastases). Study participants will receive two cycles of neoadjuvant 5 GBq [177Lu]Lu-PSMA-I&T at 6-week intervals before RPE. The primary endpoints are safety and tolerability, with an estimated study completion date of June 2027.
These studies collectively aim to evaluate the efficacy, safety, and feasibility of [177Lu]Lu-PSMA RLT in the neoadjuvant setting, potentially improving outcomes for patients with high-risk prostate cancer.
De-novo/synchronous metastatic PCaPSMA RLT may also find space in another challenging scenario of patients with de-novo metastatic PCa ineligible for SoC treatments as initially shown by Satapathy et al. in a single patient [25], and then in a pilot study in 10 de-novo/synchronous high-volume mHSPC (9/10 > 20 lesions, mainly bone) ineligible for chemo/ARPI due to cardiometabolic disorders or unwilling. Indeed, the authors observed that a maximum of 6 cycles of [177Lu]Lu-PSMA-617 plus ADT reached undetectable PSA in 50% with a median rPFS of 24 months, without any G3 or higher adverse events [26].
Further insights are anticipated from the UpFrontPSMA study, which investigated the sequencing of ADT plus 2 cycles of 7.5 GBq of [177Lu]Lu-PSMA-617 followed 6 weeks later by docetaxel (75 mg/m2every 3 weeks iv for 6 cycles) versus ADT plus docetaxel (75 mg/m2 every 3 weeks iv for 6 cycles) in 122 study participants with de-novo high volume metastatic hormone naïve disease, where [68Ga]Ga-PSMA-11 PET-expression prevailed over [18F]FDG PET-uptake. As primary endpoint, 25/61 (41%) patients in the [177Lu]Lu-PSMA-617 plus docetaxel group had undetectable PSA at 48 weeks compared with 10/61 (16%) patients in the docetaxel alone group (OR 3.9, p = 0.002), without significantly different toxicities; furthermore, after a median follow-up of 2.5 years, the reached PSA-based PFS was 30 months in the RLT arm versus 21 months in the docetaxel alone arm (HR 0.6, p = 0.04) [27].
Sathekge et al. described the use of [225Ac]Ac-PSMA-617 in a retrospective cohort of 21 mHSPC (M1b and M1c) patients who refused conventional treatments. They used a de-escalating dosage approach with an initial administered activity of 8 MBq reduced to 7, 6, or 4 MBq based on clinical, biochemical, and imaging response ([68Ga]Ga-PSMA-11 PET/CT) after each cycle. After a median of 3 RLT cycles (range 2–6) performed every 8 weeks, 20/21 patients (95%) had any decline in PSA and 18/21 (86%) showed a PSA decline of ≥ 50% (including 4 patients in whom PSA became undetectable), in the absence of any G3 or higher adverse events. A lower percentage decrease in PSA following treatment was associated with increased mortality and shorter progression-free survival [28].
AdjuvantIn the adjuvant scenario, the multicentric PROQURE dose-escalation study aims to explore the combination of SoC external beam radiation therapy (EBRT, 7 weeks), ADT (3 years) plus a single cycle of 3, 6 or 9 GBq of [177Lu]Lu-PSMA-617 (2nd EBRT week) in 18 PSMA PET-positive N1M0 PCa. The main endpoints will be tolerability and safety [29].
BCR HSPCTulipan et al. described the case of a 64-year-old patient with International Society of Urological Pathology (ISUP) grade 4 HSPC initially treated with RT and ADT, achieving a PSA nadir of 0.3 ng/ml. During the 2nd ARPI line (apalutamide after bicalutamide), the patient complained of muscle cramps, myalgia, and kidney failure, leading to the discontinuation of apalutamide and the start of a watchful waiting approach. At the time of BCR (PSA of 2.8 ng/ml), the patient underwent a [18F]PSMA-1007 PET/contrast-enhanced CT (ceCT) indicative of two highly avid lumbar-aortic lymph nodes (SUVmax 28.5 and 8.8). The patient refused chemotherapy and received a single cycle of 8.5 GBq of [177Lu]Lu-PSMA-617, resulting in a BCR-FS at 22 months after RLT [30].
In another case, Demirkol et al. reported data from a young ISUP 3 HSPC patient (56 years old) initially treated with brachytherapy (PSA nadir 1.4 ng/ml). At the time of BCR (PSA 4.4 ng/ml), a PSMA PET/magnetic resonance imaging (MRI) demonstrated the presence of highly avid local recurrence in the right prostatic lobe. However, due to medical (previous major abdominal surgery for rectal cancer), physical (obesity), and social factors (young and recently married), the patient was considered ineligible for/refused other treatments, thus receiving a single cycle of 5.8 GBq of [177Lu]Lu-PSMA-I&T followed by a BCR-Free Survival of 24 months [31].
In a pilot study, Privè et al. prospectively assessed 10 BCR participants after local therapy, considered with low-tumor burden at [68Ga]Ga-PSMA-11 PET/ceCT (≤ 10 positive lesions). All patients were treated with 2 cycles of [177Lu]Lu-PSMA-617 at 3.7 + 3 or 6 GBq according to dosimetry and eventual toxicity after the 1st cycle. Indeed, each cycle included single-photon emission computed tomography (SPECT)/CT at 1, 24, 48, 72, 168 h post-RLT (3D dosimetry following MIRD scheme), along with blood sampling at 5, 30 min, 1, 2, 3, 24, 48, 72, 168 h post-RLT for blood dosimetry. Regarding primary endpoints, at 6 months follow-up (FU), the authors did not observe any G3 or higher adverse events. Threshold radiation doses for organs at risk (OAR) were reached, while all target lesions received therapeutic radiation doses. Specifically, the salivary glands, kidneys, and bone marrow received a median total organ absorbed dose of 3.4 Gy [1.2–5.9], 4.3 Gy [3.1–6.1], and 0.15 Gy [0.1–0.2], respectively, compared to a median dose of 12.7 Gy [4.6–48.7] to target lesions. Among secondary endpoints, the authors described a PSA 50% reduction in 5/10 (1 undetectable), stability in 2/10, and 6/10 patients were PSMA PET responders. The entire cohort postponed the use of ADT while maintaining a good QoL [32].
The same patient population was analyzed in a dosimetric fashion by Peters et al., confirming that despite a dosimetric uncertainty of ~ 25% in lesions < 1 cm, the absorbed dose and organ kinetics of [177Lu]Lu-PSMA-617 in low-tumor burden mHSPC were comparable to those in high-volume mCRPC [33]. Interestingly, they observed that the “sink effect” [34], briefly described as the potential increased radiation dose in OAR especially in low-volume disease, is negligible and does not increase in later treatment cycles. Namely, the organ absorbed dose was similar or lower following the II RLT cycle, and a total [177Lu]Lu-PSMA-617 activity of at least 38 GBq is safe. Specifically, the mean organ absorbed dose resulted in 0.39 ± 0.17 Gy/GBq to salivary glands, 0.49 ± 0.11 Gy/GBq to kidneys, 0.09 ± 0.01 Gy/GBq to the liver, and 0.017 ± 0.008 Gy/GBq to the bone marrow. They also confirmed that soft tissue lesions responded significantly better to RLT than bone, as confirmed by volumetric and PSA change [33].
The same group from the Netherlands later published a retrospective study including 20 BCR patients who had undergone primary treatment and ADT but were ineligible for/refused SoC conventional treatment due to unacceptable side effects. Of these patients, 14/20 had oligometastatic/low tumor burden disease (≤ 5 mts on [68Ga]Ga-PSMA-11/[18F]PSMA-1007 PET), while 6/20 had high-volume disease; lymph node and bone metastases were present in 20/20 and 6/20, respectively. 18/20 patients underwent 1–4 cycles of [177Lu]Lu-PSMA-617, while 2/20 received 1–4 cycles of [177Lu]Lu-PSMA-617/I&T plus at least 2 cycles of [225Ac]Ac-PSMA-617/I&T (“tandem” patients). Considering a median FU of 20 months, the authors reported a median PFS of 12 m (10 m for [177Lu]Lu-PSMA-617-only, 19 m mean PFS for tandem patients) with only one relevant toxicity consisting of G3 anemia and G4 thrombocytopenia in 1 tandem patient treated with 4 cycles of [177Lu]Lu-PSMA-617/I&T plus 2 cycles of [225Ac]Ac-PSMA-I&T. Furthermore, there were 17/20 PSA responding patients, with 7/20 PSA reduction > 90%, including the two tandem patients [35].
In another prospective pilot study, Grkovski et al. included six oligometastatic (max 3 lesions) BCR PCa after primary therapy, who underwent 2 cycles of [177Lu]Lu-PSMA-617 (7.5 GBq each) and stereotactic body RT (SBRT) after 6 weeks (27 Gy in 3 fractions). In each patient, [68Ga]Ga-PSMA-11 or [18F]DCFPyL PET/CT was performed at baseline, interim (after RLT), and post SBRT, while SPECT/CT was acquired at 3, 24, and 88 h after the first RLT for dosimetric analysis. As primary endpoints, the authors did not observe any relevant toxicity within at least 4 weeks after both cycles, and RLT contribution to the mean and maximum biologically effective dose (BED) was 34 and 40%, respectively [36].
BCR HSPC recruiting/ongoing studiesSingle armThe role of RLT in early BCR PCa after RPE or RT is being evaluated in a single-centre/arm study from Vienna University. Indeed, the NCT06220188 is a phase II study recruiting 20 participants with PSMA PET-negative radio-morphological local recurrence (distant metastases are allowed; cN0, cM0/1) with PSA doubling time (PSAdt) < 12 months and Eastern Cooperative Oncology Group Performance Status (ECOG PS) 1–2. Study participants will receive 2 cycles of [177Lu]Lu-PSMA-I&T at 6-week intervals (3 + 6 GBq). Primary endpoints are PSA response > 50% (PSA50) and toxicity.
Furthermore, the ProstACT TARGET is a single-arm, phase II study exploring the radiolabeled PSMA-targeting antibody TLX591 ([177Lu]Lu-DOTA-rosopatamab) in combination with EBRT in BCR oligometastatic HSPC after definitive treatment (ISUP > 3 at histopathology). Overall, the study aims to enrol 50 participants across multiple clinical sites in Australia who will receive 2 cycles of 2.8 GBq of [177Lu]Lu-DOTA-TLX591, given 14 days apart. Inclusion criteria are the absence of prostatic-bed recurrence and the presence of ≤ 5 PSMA PET-positive pelvic lymph nodes. Specifically, participants must have at least one pelvic nodal lesion ≥ 5 mm in the greatest dimension with an SUVmax > 9 in enlarged nodes and an SUVmax > 3 in nodes < 5 mm. The primary outcome measure will be the PSA-FS, defined as the time from enrolment to PSA level increase of > 25% (NCT05146973).
Also, a phase I study will assess the safety (primary endpoint), feasibility and best dose of consolidative [177Lu]Lu-rhPSMA-10.1 after rhPSMA-7.3 (flotufolastat) PET-guided EBRT (no M1 patients) in 10 BCR patients after-prostatectomy. As secondary endpoints, patients will also undergo serial SPECT/CT and blood sample collection assessing the circulating tumor cell and dosimetry (NCT06105918).
Combination/comparison with SoCPSMAddition is an ongoing multicentric, international (19 countries) phase III study comparing (1:1) SoC (ADT and ARPI) plus 6 cycles of 7.4 GBq of [177Lu]Lu-PSMA-617 vs. SoC in untreated/minimally treated mHSPC with positive [68Ga]Ga-PSMA-11 PET/CT. The study aims to enrol 1,126 participants, who will be stratified based on several factors, including disease volume, age, and previous or planned treatment of the primary tumor. Crossover is allowed, and the primary endpoint is rPFS, with OS as a key secondary endpoint [37].
Another study of association with SoC is the phase II BULLSEYE by Privè et al., which is a prospective study recruiting 58 BCR oligometastatic HSPC after primary treatment with ≤ 5 bone/lymph node lesions at [18F]PSMA-1007 PET/CT and whole-body MRI (wbMRI) with a PSAdt ≤ 6 m. Study participants will be randomized (1:1) to receive either 2 cycles of 7.4 GBq of [177Lu]Lu-PSMA-617 every 6 weeks (plus 2 more cycles in still PSMA-avid patients at interim [18F]PSMA-1007 PET/CT) or the SoC represented by watchful wait until the initiation of ADT. Crossover to the RLT group is allowed at the end of treatment in case of clinical progression or a 100% increase in PSA from baseline. The primary endpoint is rPFS based on conventional criteria [38].
Combination/comparison with RTPOPSTAR II is an Australian phase II study recruiting 92 BCR oligometastatic PCa with positive [68Ga]Ga-PSMA-11 or [18F]DCFPyL PET after primary treatment. Study participants will be included if they have a maximum of 5 nodal/bone lesions with PSMA RADS 4–5 (low/absent PSMA uptake is allowed) with at least 1 lesion with PSMA SUVmax twice that of liver uptake. Over 24 months, study participants will be randomized (1:1) to receive either SBRT (1–3 fractions to all sites) plus 2 cycles of [177Lu]Lu-PSMA-617/I&T or SBRT (1–3 fractions to all sites), considering PSA-FS as the primary endpoint (NCT05560659).
PSMA-DC is another ambitious multicentric phase III study recruiting 450 BCR oligometastatic HSPC with positive [68Ga]Ga-PSMA-11 or [18F]DCFPyL PET after primary treatment. Unlike POPSTAR II, patients must have negative conventional imaging (CI, namely CT and bone scan - BS) for M1 disease (CI can be positive only for local recurrence) with at least 1 PSMA PET-positive CI-negative distant metastases without liver/brain involvement. Study participants will be then randomized (1:1) to SBRT plus 4 cycles of 7.4 GBq [177Lu]Lu-PSMA-617 versus SBRT alone. The primary endpoint will be the metastases-FS (RECIST1.1), while the secondary key endpoint will be the time to ADT (NCT05939414).
The LUNAR study is an ongoing monocentric study from UCLA enrolling 100 oligorecurrent HSPC. Study participants may have a maximum of 5 asymptomatic lesions outside the prostate/prostatic bed with increased radiotracer uptake on [68Ga]Ga-PSMA-11 PET/CT, with the smallest diameter ≥ 1 cm on CT or MRI or increased uptake on BS. Participants will be randomized (1:1) according to several factors towards 2 cycles of 6.8 GBq [177Lu]Lu-PSMA-I&T plus dose-adapted SBRT (based on post-RLT PSMA PET) versus SBRT to all PSMA-positive sites. The primary endpoint will be the composite PFS (PSMA PET, PSA, therapy change, death), while secondary endpoints also foresee a radiomics analysis [39].
A more complex published protocol regards the ongoing study ROADSTER, which will include (phase I n = 12, phase II n = 30) biopsy-confirmed intraprostatic recurrent PCa after RT with PSMA PET/MRI SUVmax ≥3 in the absence of any extraprostatic disease. Study participants will be randomized (1:1) to 1 cycle of 6.8 GBq of [177Lu]Lu-PSMA-I&T plus 1 high-dose-rate (HDR) brachytherapy with boost (transrectal ultrasound- and PSMA PET/MRI-guided) versus 2 HDR brachytherapy with boost. After treatment, all patients will receive a re-biopsy of the prostate for a translational study, and the primary endpoints will be safety and feasibility [40].
In Table 1 we resumed the main characteristics of the above-mentioned ongoing clinical trials using RLT in BCR HSPC. Figure 3 summarizes ongoing trials regarding PSMA-based RLT in HSPC treatment scenarios.
Table 1 Main characteristics of the described ongoing clinical trials using PSMA-based RL in HSPC Fig. 3
Main ongoing trials regarding PSMA-based RLT in HSPC
Comments (0)