
Remember me



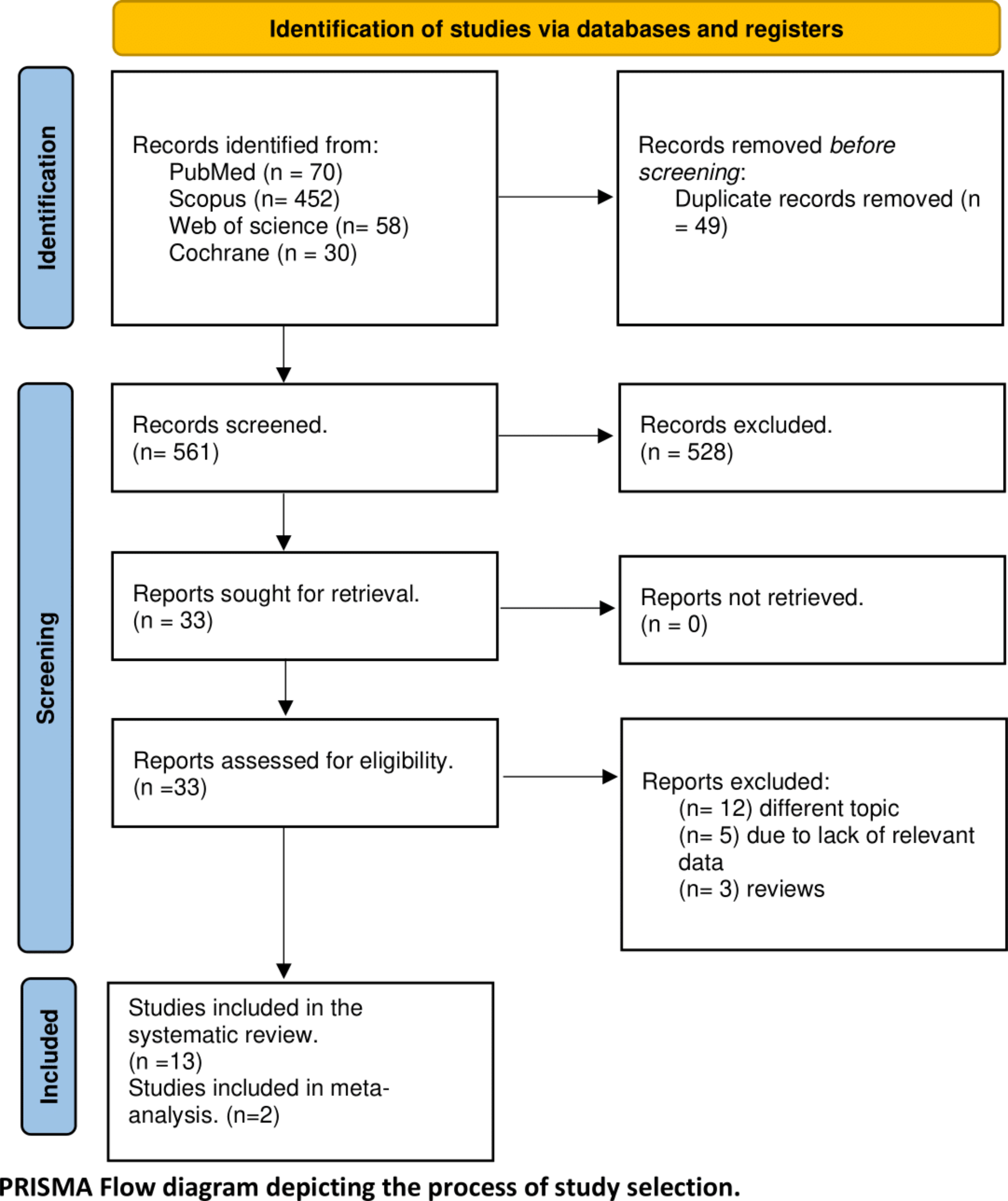


Our literature search yielded 610 results, which became 561 after the exclusion of duplicates. Title and abstract screening resulted in 33 results, and after full-text screening, we included 13 studies in our review, involving 2 in the meta-analysis (Fig. 1).
Fig. 1
PRISMA Flow diagram of the process of study selection
Characteristics of included studiesOur study included 13 studies. RCTs evaluated the efficacy of statins and combination therapies for migraine prevention, encompassing six studies from various countries with a total of 445 patients, most of them were female (86.5%). Most of our RCTs were conducted in Iran (4 studies) [25,26,27,28], while the other two were in Brazil [29] and the USA [15]. Treatment duration ranged from 4 weeks to 24 weeks. Detailed summary and baseline characteristics of the included studies highlighting the key findings of RCTs are shown in Tables 1 and 2. The rest of our included studies were seven observational studies varied in design, containing four MR studies [13, 16, 30, 31], two cohort studies [32, 33], and one cross-sectional study [14]. The Three MR studies addressed the association between the HMGCR gene and the risk of migraine, while others examined the association between statin use and migraine. Most studies were conducted in China (4 studies), with the rest from Norway, the USA, and Korea. Summary characteristics of observational studies and details about data sources are provided in Table 3.
Table 1 Summary characteristics of the included studies highlighting the key findings of RCTsTable 2 Baseline characteristics of RCTs including clinical data of migraine (frequency or days)Table 3 The characteristics of the included observational studies with details about data sources, migraine number, and key findingsRisk of bias assessmentTwo of the included RCTs had a low risk of bias and followed the standards closely [25, 26]. However, another two trials revealed a high risk of bias due to errors in the randomization method and missing outcome data [28, 29]. The latter two studies raised some concerns about possible biases in the randomization process [15, 27], for further information see Fig. 2. We applied NOS to observational studies; all studies were found to be of high quality except Buettner 2014 was of moderate quality due to self-reported data [14]. Score of each study is shown in Table 3.
Fig. 2
Results of risk of bias assessment by RoB2
Analysis of observational studiesAssociation of HMGCR gene activation with risk of migraineStudies that examined the association between the HMGCR genes and migraine have all involved overlapping datasets in their analyses. Given the risk of multiple pooling of the same group of patients multiple times, no meta-analysis could be provided for this outcome. Hong et al. found that activation of HMGCR genes was associated with an increased risk of migraine (OR = 1.46, 95% CI= [1.03, 2.07]; P = 0.035), migraine with aura (OR = 2.03, 95% CI = [1.2, 3.42]; P = 0.008), but not migraine without aura (OR = 1.04, 95% CI = [0.6, 1.81]; P = 0.876) [16]. Qu et al. used data from the International Headache Genetics Consortium (IHGC) and revealed that expression of HMGCR was associated with an increased risk of migraines (OR = 1.55, 95%CI= [1.30, 1.84]; P < 0.001). They corroborated their findings by doing an analysis of the IHGC and FinnGen datasets, showing similar results (OR = 1.38, 95%CI= [1.14, 1.67]; P < 0.001) [13]. Finally, Zhang et al. found that HMGCR was significantly associated with the high risk of migraine in both blood (OR = 1.38, 95%CI= [1.21, 1.57]; P < 0.001) and brain (OR = 2.02, 95%CI= [1.49, 2.74]; P < 0.001) [31].
Association of statins or HMGCR inhibition with risk of migraineThree studies have explored the relationship between statins or HMGCR inhibition and the risk of migraine. However, due to their different study designs, we could not conduct a meta-analysis on them. In 2014, Buettner et al. conducted a cross-sectional study examining the relationship between statin use with vitamin D status and severe headaches or migraine [14]. Their analysis of 5938 US participants demonstrated that statin use was significantly associated with a lower prevalence of severe headache or migraine (OR = 0.67, 95% CI= [0.46, 0.98]; P = 0.04), especially in patients who had serum 25-hydroxy vitamin D > 57 nmol/l (OR = 0.48, 95% CI= [0.32, 0.71]; P < 0.001) [14]. The MR study by Bi et al. supported these findings by revealing that HMGCR inhibition had a significant association with a lower incidence of migraine in the FinnGen dataset (OR = 0.64, 95% CI= [0.46, 0.88]; P < 0.001) and amarginal non-signficant association in the Choquet dataset (OR = 0.78, 95% CI= [0.60, 1.01]; P = 0.06) [30]. A combined analysis of these datasets showed a reduced overall migraine risk (OR = 0.73, 95% CI= [0.60, 0.89]; P < 0.001) [30]. Recently, a 2024 Nationwide Korean Cohort by Kang et al. further confirmed that statin use was associated with a reduced likelihood of overall migraines (OR = 0.93, 95% CI= [0.91, 0.95]; P < 0.001), particularly for migraines with aura (OR = 0.75, 95% CI = [0.65, 0.86]; P < 0.001) and without aura (OR = 0.94, 95% CI = [0.92, 0.96]; P < 0.001) [33].
Effect of statin on triptan use for migraineAccording to A nationwide registry-based cohort study by Bjørk 2023, Out of 6096 Statin-using patients, 56.71% had a 30% decrease in triptan consumption over the first ninety days of therapy, with propensity score-adjusted odds ratios of 1.28, 95%CI= [1.19, 1.38) [32].
Analysis of clinical trialsStatins efficacy on migraine frequency and daysTwo RCTs reported MMF with 93 statin users and 91 controls. The findings demonstrated that statins were significantly associated with reduced MMF versus placebo (MD= -3.16, 95%CI= [-5.79, -0.53]; p = 0.02), albeit with substantial heterogeneity (P = 0.03; I2 = 79%) due to the variability of treatment regimens in each study (Fig. 3). This aligns with the results reported by Sherafat in 2022 which indicated that the combination of atorvastatin and nortriptyline reduced the risk of headache attacks by 46% when compared to nortriptyline alone (OR = 0.54; 95%CI= [0.34, 0.85]; P = 0.007) [28]. Additionally, Buettner et al. revealed that simvastatin plus vitamin D significantly reduced MMD compared to placebo in adults with episodic migraines (MD = -11.33, 95%CI= [-14.20, -8.46]; P < 0.001) [15].
Fig. 3
Meta-analysis of statins efficacy on monthly migraine frequency
Statins compared to other drugsIn 2008, Medeiros et al. compared Simvastatin 20 mg to Propranolol 60 mg and found that both simvastatin and propranolol significantly reduced MMD in women with Simvastatin showing greater decrease (MD = -20.65, 95%CI= [-21.06, -20.24], P < 0.001) than propranolol (MD = -14.85, 95%CI= [-15.44, -14.26], P < 0.001). In addition to reducing the frequency of migraine attacks, 88% of participants taking propranolol and 83% of those taking simvastatin experienced over a 50% reduction in migraine frequency [29]. Lately, in 2018, Hesami et al. randomized 46 patients to Atorvastatin (40 mg daily) and 36 patients to Sodium Valproate (500 mg daily) and found the numbers of patients with more than 50% reduction in the number of attacks (responder rate) were 30 (65.2%) in atorvastatin group and 26 (72.2%) in sodium valproate (P = 0.499), and both treatments reduced intensity, and duration of migraine attacks with less adverse events observed in Atorvastatin group, suggesting that atorvastatin could be a good alternative for migraine prophylaxis [26].
Statins safety and tolerability for migraineThe included studies demonstrated that statins maintained a favorable safety profile, showing results comparable to those of the control groups. At the same time, the event rate of all adverse events for statins was markedly less than sodium valproate (32% vs. 66%). However, the heterogeneous nature of the arms of the studies included in the meta-analysis precluded the conclusion of any significant adverse events to compare between the statin group and other groups. We also provided a summary of all adverse events in Table 2.
Comments (0)