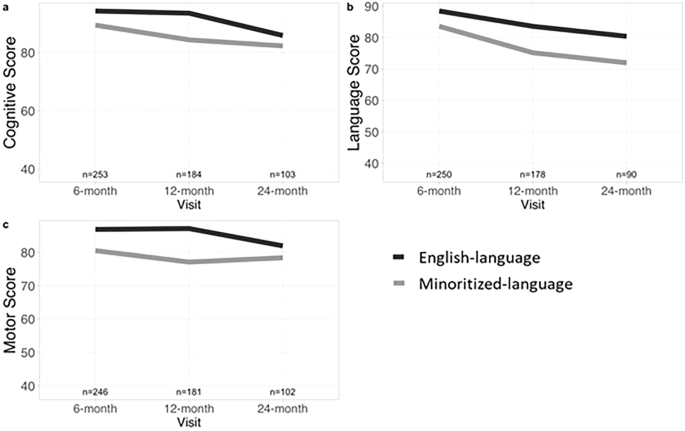
In our study of 253 high-risk neonates, we identified disparities in developmental outcomes with a widening gap in language skills by 24 months corrected age for the minoritized-language infant group. Interestingly, our exploratory analysis revealed that infants in the lower COI level group had significantly lower language scores at the 24-month visit compared to infants in the higher COI level group. This finding parallels the gap in language scores between minoritized- and English- language groups and highlights the connection between language-access and opportunity. Reasons for the disparities found between minoritized- and English-language families in this study may include barriers to accessing care and lack of language concordance between provider and patient [17, 24,25,26,27,28]. In addition, lower neighborhood opportunity level may have further impacted disparities in language outcomes as indicated by the results of our exploratory analysis. Minoritized-language families experiencing lower socioeconomic opportunity may face compounding inequities in care. Our findings that lower COI was associated with lower language scores at 24 months corrected age aligns with studies showing an association between lower socioeconomic status and decreased language enrichment [29].
Two studies of high-risk populations, one examining mother’s milk provision to NICU infants and one examining access to services for children with autism, found that parents speaking a minoritized language faced greater challenges in accessing support services and therapies [17, 24]. Parents who do not speak the majority language may be afraid to raise concerns and pursue evaluations and services due to factors such as lack of knowledge and resources, lack of empowerment, community mental health stigma, and worry about burden on the family [25, 26]. Barriers to logistical factors such as scheduling appointments and arranging transportation also prevent connection to care [25]. These factors may impact follow-up care and connection to early intervention services, which are correlated with positive health and developmental outcomes for this population [30, 31].
In addition, service quality and outcomes may be impacted by patient-provider racial, cultural, and language concordance [28, 32, 33]. A global dataset analysis revealed that being from a minority language-speaking household was associated with lower odds of on-track developmental scores compared to being from majority language-speaking households [27]. Other studies have shown that lack of patient-provider racial and language concordance and associated sense of connection and safety may affect rapport, engagement, and performance on assessments [25, 28, 33]. Families speaking a minoritized language have also perceived interpretation services to be inadequate due to limited availability of in-person interpreters or insufficient training of interpreters available in the medical settings [25]. Another consideration is whether the differences in language scores between children of majority and minoritized language speakers are truly a reflection of disparities in outcomes or rather a reflection of bias introduced by performing English language-based testing through an interpreter [14]. In addition, assessment of health literacy using validated tools can also be helpful in identifying additional communication needs [34]. These issues highlight the importance of staffing diverse, multi-lingual providers and providing access to appropriate supports, including reliable interpreters who can navigate both linguistic and cultural divides [32, 33].
Our study had several strengths. First, we were able to examine our cohort through longitudinal time points from NICU discharge to 24 months of age corrected. This allowed us to monitor the progression of developmental outcomes and make comparisons over time. Next, for COI, we used address rather than zip code data. Zip codes, designed by the United States Postal Service for efficient mail delivery routes, have been found to be less reliable than geocoded data and tend to overestimate neighborhood opportunity for Black and Hispanic children while underestimating neighborhood opportunity for White children [35, 36]. Lastly, despite a significant difference in COI levels between minoritized- and English-language groups, differences in developmental outcomes persisted when the sample was adjusted for COI, strengthening the association between maternal primary language and infant developmental outcomes.
There were several limitations to our study. One was loss to follow-up at subsequent visits. Between 6- and 24-month visits, the minoritized-language group surprisingly had a higher follow-up rate compared to the English-language group. Ideally, the follow-up rate would have been measured from NICU referral if that were available. Factors found to be associated with loss to HRIF follow-up include barriers such as lower maternal education level, greater distance from clinic, non-English primary language, Black non-Hispanic race, very low neighborhood opportunity level as well as indicators of lower medical severity such as shorter length of hospitalization and higher gestational age [37,38,39]. While we did not find a difference in language, gestational age, and birth weight for those who followed up and those that did not, there may be undetected confounding effects from individual socioeconomic factors that were unavailable in our chart review. We used COI as a proxy for socioeconomic status, but it is determined by one’s address at a single point in time and may not reflect long-term opportunity. A family’s opportunity level may fluctuate over time and can be influenced by individual factors such as household income and time in poverty [40]. Another limitation was missing birth and NICU hospitalization data, often from outside referrals, limiting our ability to utilize neonatal medical severity indices, which would have allowed us to more precisely compare medical severity between the minoritized- and English-language groups [41]. We were at least able to correct for gestational age, which has been strongly correlated with infant morbidity and mortality [42]. Next, although our therapists performing BSID assessments were highly experienced clinically, we could not ensure interrater reliability, given that this was a retrospective study so there may have been variation between assessors. Additionally, interpreters were used for non-English assessments, which added additional time to the assessment and may have altered the standardization of administration. Lastly, the Bayley kits used were in English and consideration for impact of language and cultural differences on developmental testing outcomes is important in the interpretation of these results [33].
Our findings demonstrate disparities in developmental outcomes, particularly in language skills, for infants of mothers who speak Spanish or another minoritized language in the United States. While this group appeared to catch up to their English-language counterparts in the cognitive and motor domains by 24 months corrected age, a difference in language domain scores persisted. Few studies have examined disparities correlated with maternal primary language. These findings underscore the need for further research to inform targeted interventions to address disparities in developmental testing and outcomes associated with minoritized primary language and low socioeconomic opportunity. Addressing health inequity is an important goal for neonatal care, which does not end at discharge from the NICU.

Comments (0)