Our primary aim was to learn from health care workers about their experiences in DHR’s NICU. Through our semi-structured interviews and subsequent qualitative analysis, we uncovered four themes representative of the insights shared by the participants.
Workflow around interpretation
Most participants report the ability to communicate with patient families in both English and Spanish. Bedside nurses described an informal system for communicating with SS families in which a NSS bedside nurse asks a SS provider to communicate with his or her patient’s parents directly while the NSS nurse takes over another responsibility for the SS provider. This workflow differs from conventional interpretation in many ways.
In most hospital settings, communication with SS patients and families is facilitated through professional medical interpretation services accessed on an as-needed basis. This service, provided via in-person interpreter, phone call, or videoconference, is typically external to the clinical care team, meaning that it might not provide the immediacy, continuity, or flexibility of communication needed in a NICU environment with many SS families. Additionally, dedicated interpreters conventionally serve as intermediaries between SS parents and NSS staff. This NICU’s informal system facilitates direct communication between SS parents and SS staff.
This informal system mitigates some challenges inherent to the conventional system of interpretation as SS staff in this NICU are always present and provide direct communication with SS parents and caregivers without an intermediary. Still, other problems, such as that providers tend to overestimate their Spanish fluency when they are asked to self-report [13], may persist. In this NICU, it is possible that this issue remains given that only some of the self-identified SS providers are certified medical interpreters.
Another aspect of this system worthy of further investigation is the consequences, if any, of the trading of responsibilities described by participants. It could be that the provider who temporarily assumes responsibility over another’s patient for the purpose of communication with that patient’s family may not be as familiar with the medical condition of that patient as the original NSS nurse. The effect of this complication on the quality of communication with SS families compared to English-speaking families remains unknown and warrants additional research.
Studies show that the infants of Spanish-speaking caregivers are at increased risk for several diseases common in the NICU, suggesting the importance of complete integration of Spanish-speaking families in the healthcare system [14]. By leveraging the availability of SS staff, this NICU aims to accommodate SS families. Additional evaluation of this system’s strengths and limitations can provide insight into the general effectiveness of this model of accommodation. Programs that reward SS providers directly for receipt of their formal interpreter certification and indirectly for their ongoing efforts as interpreters may support this workflow and alleviate negative feelings associated with SS providers’ increased responsibilities while ensuring high-quality communication with SS families. SS providers who opt not to participate in the certification process or whose language skills leave them ineligible for certification should not be discouraged from speaking to SS families in an informal context. Studies with adult patients find that professional interpretation successfully facilitates health education for limited English proficient patients; however, professional interpretation did not improve their impression of the quality of the interpersonal care they received [15, 16], suggesting that building rapport and increasing the frequency of communication with patients’ parents and caregivers by SS providers may be beneficial even when dedicated interpreters are involved in conversations regarding the patient’s medical status or prognosis.
In sum, with adequate incentives, formal certification requirements can support, rather than hinder, this model of accommodation involving direct communication between SS families and providers.
Cultural concordance between patient families and staff
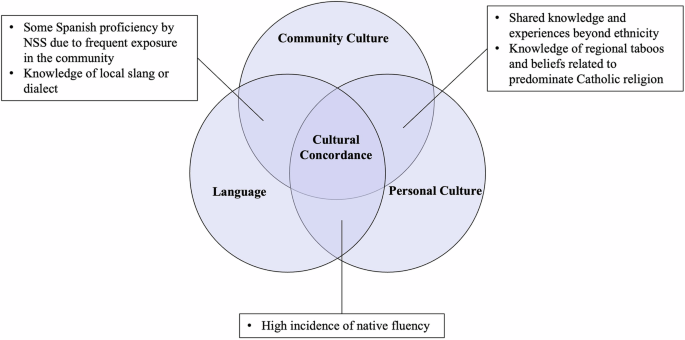
Another important theme is cultural concordance between patient families and providers. This study revealed the perceived importance of several distinct aspects of culture: community culture, personal culture, and language (Fig. 1). Each aspect can work alone or in combination to create a sense of shared experience and facilitate effective communication. For example, local knowledge contributes to cultural concordance between two locally born individuals even when they do not share the same ethnicity. Meanwhile, individuals who share ethnicity and language may be in cultural discordance if one does not know about local taboos, perspectives, and slang. Neither ethnicity, language nor local knowledge alone guarantees cultural similarity; experiences shared by participants illustrate how all three concepts can work together to create a sense of relatability and trust between patient families and providers.
Additional work should focus on whether having a mostly local workforce contributes to a feeling of shared experience and trust between parents and providers, as well as if this feeling of cultural concordance can be fostered in non-local, non-Hispanic, or NSS providers via cultural education, structured interactions with community members like former patients, or other programming. Whether these types of cultural concordance, perhaps through increased trust and communication and therefore increased caregiver preparedness for discharge or facilitated parent-infant interactions in the NICU, confer a measurable clinical benefit to patients is also deserving of additional study.
Accepted and appropriate support for families
Participants perceived that the availability of comprehensive, culturally competent mental health care from a doctoral-level psychologist contributes significantly to this NICU’s success. While the majority of NICUs nationally provide some form of mental health screening for parents, most rely on social workers, nurses, or other non-psychologists to deliver these services [17]. Community-based NICUs are more likely than academic centers to lack even routine mental health screening for parents and caregivers [17]. In this context, DHR represents a relatively rare example of a community-based NICU offering in-unit, comprehensive mental health support from a doctoral-level psychologist, an approach that aligns with the National Perinatal Association’s recommendations for NICUs with 20 or more beds [18].
High-quality, easily accessible mental health care may be especially critical for this population given the elevated rates of postpartum depression (PPD) among Hispanic mothers [19], who are also among the least likely to access postpartum mental health care due to a variety of structural barriers [20]. Untreated PPD and other perinatal mental health conditions are known to negatively affect infant health and development [21]. The effect of a dedicated mental health specialist providing routine, on-site care to a predominantly Hispanic population of NICU parents and caregivers warrants further investigation in part because access to these providers is a modifiable and potentially replicable component of NICU care.
As with NICU mental health services, the presence of lactation consultants (LCs) and high-risk infant follow-up clinics for NICU families is generally considered standard practice. It is the specific structure and delivery of these services at DHR, which was emphasized by participants, that is notable. Fewer than half of NICUs nationwide employ a board-certified lactation consultant dedicated exclusively to the NICU [22], and little is known about the availability of language-concordant lactation support for SS mothers in non-academic settings. At DHR, participants reported that the SS LC and follow-up clinic staff assist families in accessing public health programs to obtain breast pump supplies and specialized formula. These efforts extend beyond the traditional scope of clinical care and may play a role in promoting good clinical outcomes for patients. Future research should aim to clarify this clinical effect, as the delivery of these supports represents a modifiable component of care that can be fine-tuned to serve other distinct populations.
Staff consistency
Participants reported positively about the effects of physician and nurse longevity. It is known in other settings that increased nurse tenure leads to shorter lengths of stay [23]; however, this aspect of care remains under-studied in the NICU setting even as retention of nursing staff in a variety of settings remains a significant challenge [24, 25]. In this study, the majority of participants reported working in this NICU for more than ten years. Additional work should focus on what has facilitated staff longevity so that other NICUs with significant staff turnover can attempt to replicate these features. This work is especially warranted considering the increase in travel nursing and other changes to the nursing workforce during and after the Covid-19 pandemic [26].
Study limitations
As with all qualitative research, the findings of this study are context-dependent and may not be generalizable to all NICU settings or patient populations. The data reflect the experiences and perceptions of participants within a single hospital that serves a predominantly Hispanic community in a medically underserved region. Certain features of this NICU such as the availability of Spanish-speaking staff and providers with a high degree of cultural concordance with patient families may not be present nor replicable in other institutions. Additionally, in settings with greater linguistic or cultural diversity among patients and families, even the aspects of care identified here as modifiable may be more difficult to implement or may require different approaches.

Comments (0)