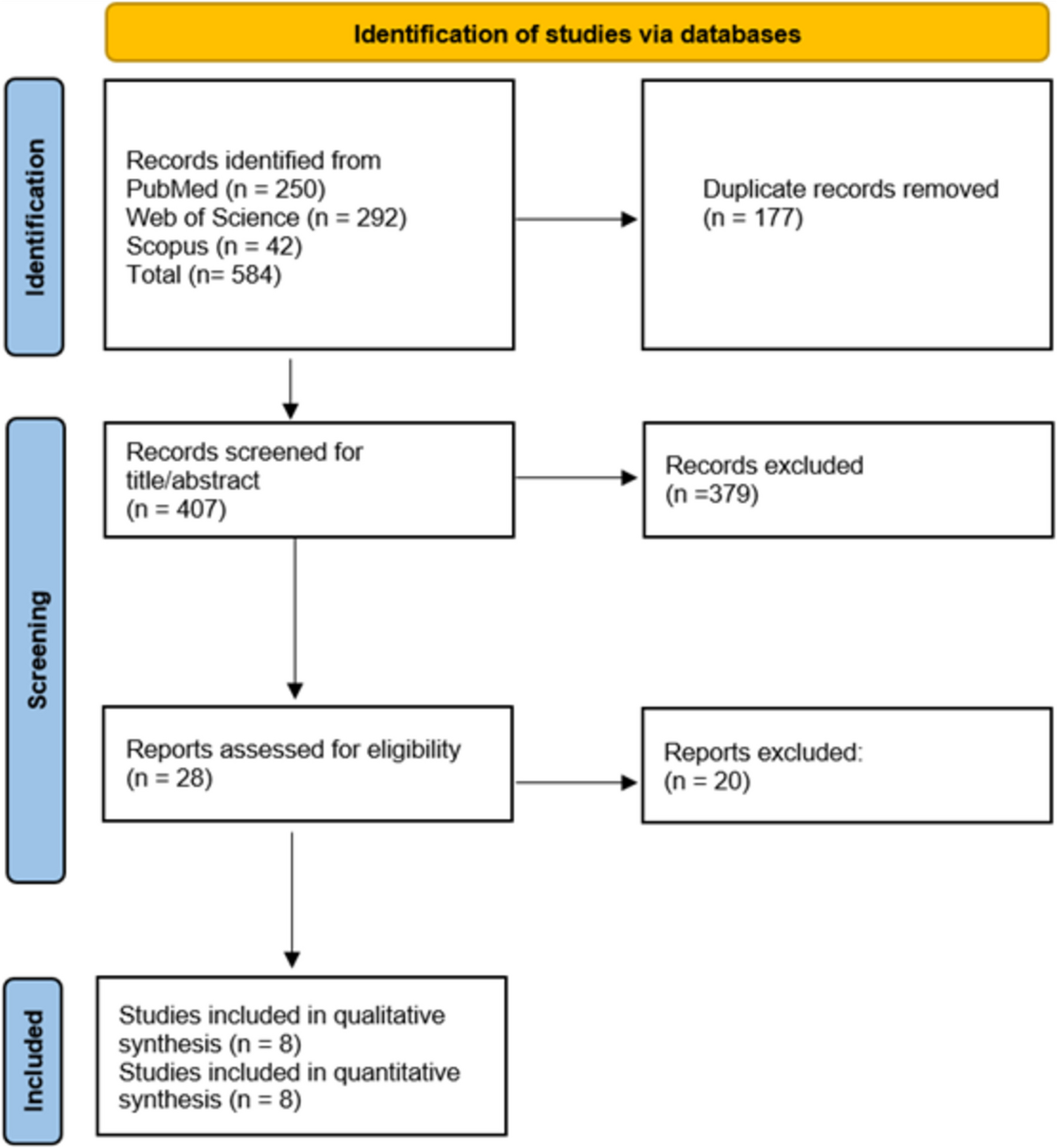
This meta-analysis rigorously encompassed up-to-date literature and pooled eight studies with a total of 376 patients to provide robust evidence demonstrating that lomitapide considerably improved lipid levels in the homozygous familial hypercholesterolemic patient with HoFH. Our study demonstrated a noticeable LDL-C reduction of 49.27%, accompanied by a decrease in total cholesterol (TC) (−46.05%) and non–HDL-C (−51.31%). In addition, apolipoprotein B (apoB) was reduced by 51.01%, reflecting Lomitapide's capacity to reduce atherogenic lipoproteins, significant drivers of cardiovascular risk [26]. Conversely, HDL-C levels remained relatively unchanged, with a minimal reduction of 4.63%. TG and VLDL-C, however, experienced considerable reductions of 46.39% and 48.73%, respectively. These reductions are of clinical importance as lowered triglycerides have been found to be associated with lowered risk for large vascular events, even when risk adjustment is performed for LDL-C reduction in HoFH patients [27]. In terms of safety, side effects from the included trials were generally tolerable. However, 14% of patients withdrew from the trials due to side effects. The most common adverse reactions were diarrhea (31%), nausea (22%), and infections (20%).
Before the introduction of contemporary lipid-lowering therapies, patients with HoFH often presented with extremely elevated LDL-C levels, ranging from 13–27 mmol/L (500–1000 mg/dL) [1, 28, 29]. While statins remain a cornerstone of therapy, their effectiveness in HoFH is often limited due to insufficient LDL receptor activity [30]. Similarly, PCSK9 inhibitors, though revolutionary in general hyperlipidemia management, show reduced efficacy in HoFH, with only 23% LDL-C reduction over 48 weeks [31]. Given this context, the LDL-C reduction achieved with Lomitapide may lead to improved life expectancy and lower cardiovascular event rates in HoFH patients [32, 33]. While lipoprotein apheresis is another treatment option capable of acutely reducing LDL-C by over 70%, its effects are short-lived [34]. In contrast, Lomitapide offers sustained long-term control of LDL-C levels [35]
Regarding safety, our findings of 14% discontinuation due to adverse events appear lower than previously reported in early trials [36], where gastrointestinal disturbances were more prevalent (e.g., diarrhea in 79%, nausea in 65%, and GI symptoms overall in 93%). However, findings from longer-term real-world studies, consistent with clinical trial experience, suggest that Lomitapide is associated with a risk of hepatic steatosis. Liver imaging has demonstrated a moderate increase in hepatic fat content, typically accompanied by normal liver stiffness [37]. In pediatric populations, one study reported that transient elevations in liver function tests, exceeding three times the upper limit of normal, may occur. These changes are generally manageable through temporary dose reduction, followed by gradual re-titration to the previous dose [38]. Notably, hepatic steatosis may develop with or without concurrent elevations in liver enzymes, particularly transaminases [39]. Encouragingly, emerging long-term real-world evidence shows that Lomitapide can maintain significant LDL-C reductions for up to seven years without discontinuation, supporting its potential as a durable treatment option [40]. Nevertheless, further studies are needed to evaluate long-term adherence, explicitly reporting the duration of therapy and reasons for discontinuation, if any, to better inform clinical decision-making. Additionally, the Homozygous Familial Hypercholesterolemia International Clinical Collaborators (HICC) consortium, which was not included in our analysis due to the case-based nature of reporting, provided perspectives of Lomitapide use in real-world settings in a multinational cohort. While the consortium findings are not limited to Lomitapide, it did highlight the increasing utilization of Lomitapide, most often in combination with other therapies, including statins, ezetimibe and PCSK9 Inhibitors, with higher rates of effectiveness than conventional treatments alone. Despite this, Tromp et al., reported that out of 751 patients across 38 countries, only 14.7% were successfully treated with Lomitapide, with minimal to no usage in low- and middle-income countries, which suggests geographic disparities leading to significant gaps in drug usage due to global accessibility, as a result of high cost, lack of availability or guideline enrolment and clinician unfamiliarity in the global south regions [2]. Furthermore, in another report by Mulder and Tromp et al., sex-based disparities were found, with female patients having a more notably delayed diagnosis, which contributed to delaying the initiation of appropriate treatment, including Lomitapide, and affecting these patient outcomes [41].
This single-arm meta-analysis, to the best of the authors'knowledge, is the first to evaluate the efficacy and safety of lomitapide in HoFH patients. It encompasses real-world and clinical trial evidence across adult and pediatric patients, and this provides a snapshot of lomitapide's impact. Strengths of the analysis are the use of standardized outcome measures, rigorous methodology, and inclusion of studies with varying populations and treatment histories. However, there is no control group to be drawn upon, and causality establishment is restricted; the overall quality of the included studies was mostly fair, but some were rated as poor. The other restrictions are small sample sizes and variable follow-up reporting. Future research needs to focus on well-executed randomized controlled trials of longer duration with larger and more representative cohorts. Furthermore, ongoing publication of long-term efficacy and adverse events, particularly hepatic-associated ones, will be key to guiding clinical decision-making and optimizing the therapeutic use of lomitapide.





Comments (0)