Key findings
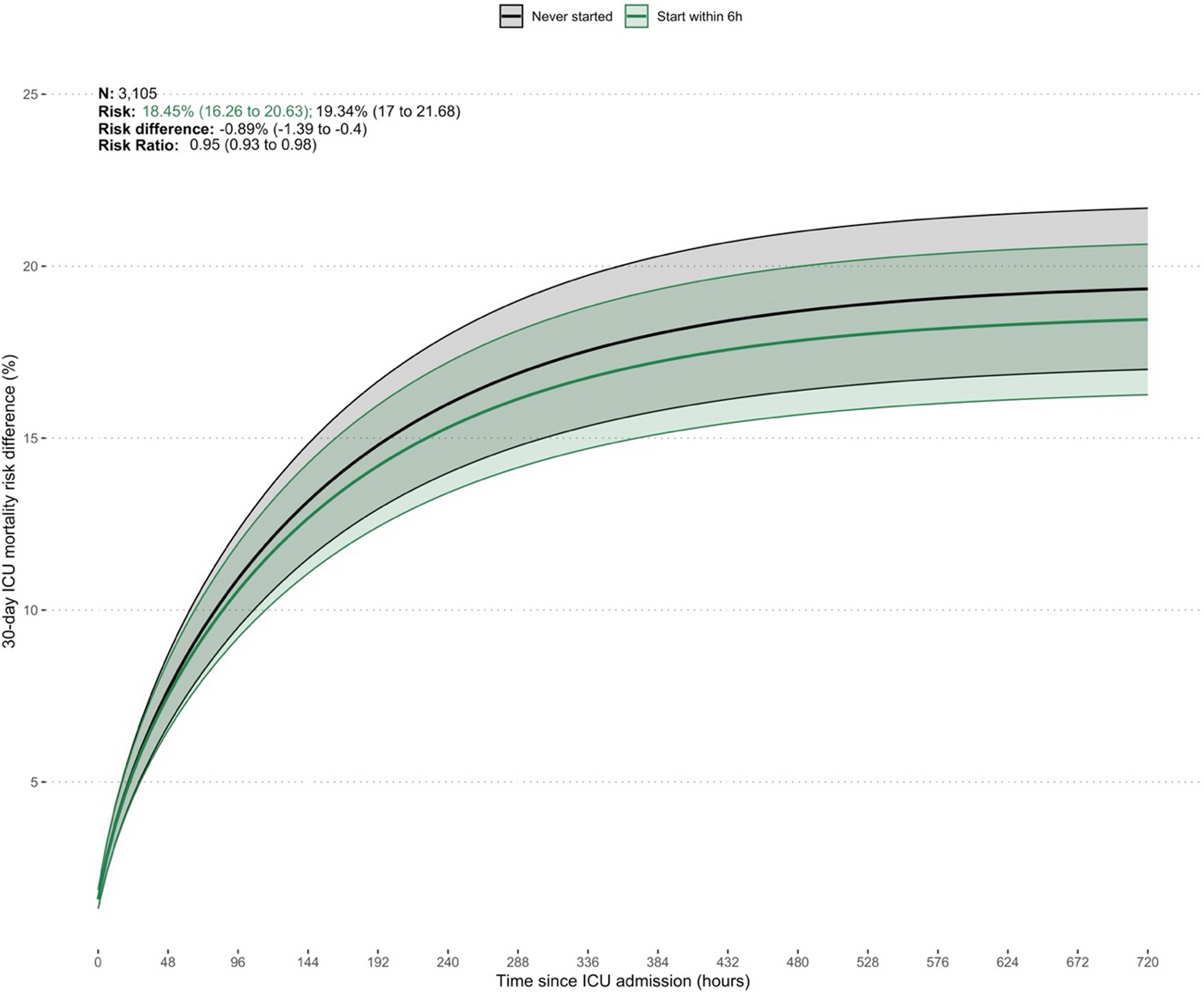
In this study, we emulated a hypothetical target trial and found that, after adjustments, patients with septic shock who received early adjunctive vasopressin therapy (≤ 6 h) had a lower risk ratio for 30-day ICU mortality than patients who never received vasopressin or who received late vasopressin therapy (> 6 h). Moreover, this effect was progressively diminished as vasopressin start occurred after 12 h, 18 h and 24 h. Similarly, the beneficial mortality effect was strongest when the NED was 0.1 µg.kg−1.min−1 and diminished as the NED at the start of vasopressin moved to 0.125 and then 0.2 µg.kg−1.min−1 and was absent at 0.25 µg.kg−1.min−1 or above. The beneficial effect of vasopressin was pervasive and significant in all groups (high or low lactate, ventilated or not ventilated, APACHE score < 80 or ≥ 80).
Relationship to previous studies
There are limited data available on outcomes relating to early initiation of adjunctive vasopressin therapy in septic shock patients. The only multicentre randomised controlled trial to consider a timing threshold, the VANISH study, enrolled patients within six hours of shock onset [4]. Similar to our patient cohort, these patients had a ‘low dose’ vasopressor requirement with a median norepinephrine dose of 0.16 µg.kg−1.min−1. Furthermore, in the VANISH study, less than 60% of patients were mechanically ventilated and the median lactate was 2.3 mmol.L−1. This study did not identify any significant difference in mortality rates between the examined groups, in contrast with our results. However, the VANISH study included vasodilatory shock patients who are known to have different outcomes when compared to septic shock [16]. In addition, the study was underpowered, limiting the reliability of its conclusions. Notably, the study did not observe a beneficial effect of hydrocortisone treatment, a finding that contrasts with results from larger randomized controlled trials such as APPROACHS and ADRENAL, which have suggested its beneficial effects regarding ICU length of stay, duration of shock, and duration of mechanical ventilation [33, 34].
A signal of benefit for early adjunctive vasopressin use compared with late initiation has been assessed in retrospective studies [5, 9]. White et al. showed that, among septic shock patients, later time to vasopressin initiation was independently associated with hospital mortality [9]. This is consistent with our finding of higher mortality risk with late vasopressin initiation. However, in our study, we extended such findings by target trial emulation and found that compared to no vasopressin use, early vasopressin was associated with a decreased risk of death.
Sacha et al.’s study showed a linear association between hospital mortality and lactate concentration at time of vasopressin initiation [5]. Furthermore, the odds of death increased with increasing lactate concentration at vasopressin initiation when time from shock onset to vasopressin initiation increased. However, there was no independent association between hospital mortality and timing of vasopressin initiation. These results suggest a longer duration of hyperlactatemia without adjunctive treatment (and possibly ‘decatecholaminisation’) may be detrimental [1]. Similarly, in our study, the beneficial effect of early vasopressin was particularly strong when the lactate was > 4 mmol.L−1. Thus, a lactate > 4 mmol.L−1, despite a norepinephrine-equivalent infusion dose ≤ 0.25 µg.kg−1.min−1, may be an important clinical trigger to commence adjunctive vasopressin in the first six hours of septic shock management.
Kalimouttou et al. have shown that in patients experiencing septic shock, a reinforcement learning model suggests the earlier and more frequent administration of vasopressin [35]. Key factors influencing the decision to start vasopressin according to this model include the duration since shock onset, the SOFA score, the norepinephrine dosage, and the serum lactate levels at the time of vasopressin administration. These findings align closely with our results.
Implications of study findings
To our knowledge, this is the first target trial emulation of early adjunctive vasopressin use in septic shock patients. This is an important cohort of patients to consider given the time critical nature of septic shock treatment and current international guidelines, which do not advocate adjunctive vasopressor therapies below a norepinephrine base infusion dose threshold of 0.25 µg.kg−1.min−1.
Our study provides important findings to help better inform patient selection and interventions for a prospective randomised-control trial for early adjunctive vasopressin use in septic shock. It implies that early vasopressin therapy may be desirable. Moreover, it implies that initiation at lower doses of norepinephrine administration (> 0.125 µg.kg−1.min−1 but < 0.25 µg.kg−1.min−1 of norepinephrine tartrate) than currently recommended by the Surviving Sepsis Campaign guidelines (between 0.25 and 0.50 µg.kg−1.min−1 of norepinephrine base) may also be desirable. In addition, it suggests that patients with a lactate > 4 mmol.L−1 and patients on mechanical ventilation may be easily identifiable candidates in whom early administration of vasopressin may be particularly beneficial. Finally, our results highlight the limited magnitude of effect that investigators should expect when designing such trials.
Strengths and limitations
This study had several strengths. In particular, this target trial emulation cohort was sampled from a large, comprehensive ICU patient database covering nearly all ICU admissions in a large state of Australia. This population is generalisable to the wider Australian population and likely to other high-income countries. Moreover, our highly granular study data was electronically extracted from a mature clinical information system in daily clinical use at all twelve study sites. There were minimal missing data points. In addition, the methods to emulate a hypothetical target trial, selection and adjustment for confounding variables and strict eligibility criteria minimise immortal time bias and confounding by indication and prespecified sensitivity analyses were performed with results consistent with our primary analysis. Finally, our study design encompassed all patients with the condition of interest, avoiding the selection bias frequently found in randomized controlled trials.
We acknowledge some limitations. First, the groups differed significantly at baseline, with the treatment group having a higher severity of illness. This raises the possibility of residual confounding. However, the adjustments performed with target trial emulation methodology are likely to have addressed such differences. Second, we do not have data to explain why clinicians commenced vasopressin early or late in this patient cohort. Therefore, despite being reduced by the study design, there may still be confounding factors due to vasopressin being given to patients whom clinicians judge most likely to survive. However, early initiation of vasopressin may also easily indicate greater illness severity and such indication bias may have actually decreased the true magnitude of the benefits associated with vasopressin. Third, although there is a significant effect across all subgroups, the severity of patients may impact outcomes. Fourth, we only admitted patients diagnosed with septic shock during the first six hours of their ICU stay, which limits the applicability of these results to other groups. Fifth, a time-related effect might have affected our results as we covered a six-year period. Finally, despite the imputation method we performed, missing values may have biased our results.


Comments (0)