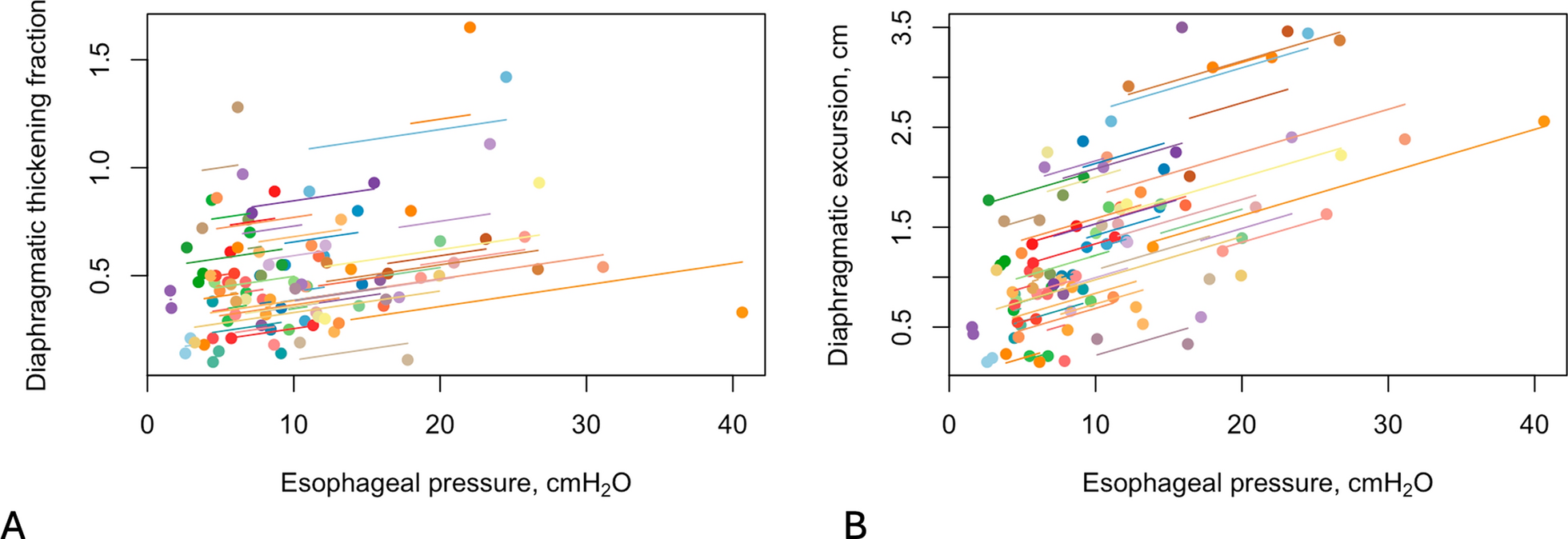
This study aimed to evaluate Dex and Tfdi as non-invasive estimates of breathing effort under inspiratory resistive load. Such conditions mimic common critical care scenarios, including endotracheal tube obstruction (due to secretions, clots, or plication) and post-extubation airway edema [23, 24]. Our findings showed that Dex exhibited a significant but weak to moderate correlation with ΔPes, ΔPdi, and PTPes. However, both Dex and Tfdi increased significantly under IRL. Additionally, Dex significantly differed between patients who were successfully weaned and those who failed, while Tfdi showed no such distinction.
In this study, the correlations between Dex and indices of breathing effort were weak to moderate, and there was an overlap in values between weaning success and failure, limiting its predictive accuracy. These results can be explained by the fact that; a) ΔPes and ΔPdi are the product of the combined activation of all inspiratory muscles [36] and not only of the diaphragm, b) Dex does not capture isometric contractions of the diaphragm, during which there is no measurable excursion, whereas the pressure–time product of esophageal pressure (PTPes) does account for this [30] and c) under conditions of increased resistive load, the diaphragm may not always be the primary contributor to inspiratory pressure generation, further complicating its relationship with breathing effort [37, 38].
Moreover, Dex is influenced by the interplay between respiratory mechanics, lung volumes, and intrathoracic/intra-abdominal pressures [5, 6, 17, 22]. In addition, the pattern of respiratory muscle activation varies significantly between subjects [36, 39, 40] and leads to variable rib cage and abdominal displacement combinations. Consequently, in Dex there is an increased interpatient variability. Based on these, in spontaneously breathing patients under a resistive load, as our population, Dex may be used as a monitoring tool, assessing temporal trends, but not exact values of breathing effort, and assisting in weaning outcome predictions.
TFdi did not correlate with indices of breathing effort, even though it increased when IRL was applied. Furthermore, it did not differ between patients who succeeded and failed weaning. This does not mean that our study suggests that TFdi is not a helpful index for weaning. There are studies where Tfdi correlated significantly with breathing effort [14, 15, 19, 20] and with weaning outcomes [7,8,9]. However other studies that align with our results [10, 13, 16,17,18], showed weak or no correlation between Tfdi, breathing effort and weaning outcomes. Finally, in a previous study [41], TFdi increased during the SBT. While TFdi may have risen even without IRL, the strong temporal association between IRL application and increases in Pes, Pdi and Tfdi may suggest a causal relationship.
Population-related and methodological factors may have contributed to these differences. Prior research has highlighted significant variability in respiratory muscle activation patterns, both in critical care patients [15,16,17, 21] and in healthy individuals [36,37,38,39,40]. This variability in respiratory muscle recruitment could explain the inconsistent relationship between TFdi and pressure output [15,16,17]. Specifically, in critical care patients with diaphragmatic dysfunction, an increased activation of extra-diaphragmatic muscles has been observed [15, 21]. Our data may suggest a reduced contribution in respiratory pressures from the diaphragm. This could be attributed to either diaphragmatic dysfunction and/or an increase in extra-diaphragmatic muscles as compensation [15, 21], or to preferential use of the respiratory accessory muscles [36, 39]. In this cohort, depending on the definition used [4, 5], diaphragmatic dysfunction ranged between 50 and 80%, which aligns with the reported rates in the literature [42]. Our population consisted of critical care patients who had been ventilated for longer periods than those in previous studies [7, 14, 15, 19], increasing the likelihood of respiratory muscle dysfunction [43] and possibly weakening the association between TFdi and pressure generation [15]. Unfortunately, the activity of the extra-diaphragmatic muscles was not assessed and as such we cannot provide further insight at this point. Furthermore, different resting lung volumes may have been an additional factor introducing interpatient variability in the diaphragmatic pressure-generating capabilities [44] and should be considered for in future investigations. Other technical issues in respect of the measurement, such as inclusion or not of the pleura, might have also affected the relationships between sonographic indices and breathing effort which were found in the present study [5, 17]. Even though the zone of apposition is considered the place of maximal thickening [45], the force-generating capacity of the diaphragm is not uniform [46] and as such interpatient variances cannot be ruled out [47]. Consequently, the visualized part of the diaphragm might not accurately reflect the function of the whole muscle.
Furthermore, while in almost all successfully weaned patients Tfdi was above the usual cut-offs (> 30–35%), the weaning failure group displayed a wide range of Tfdi values, with the average being above the usual thresholds [4, 7, 9]. This suggests that while TFdi < 30–35% is strongly associated with weaning failure, as previously reported [7], values above this threshold do not necessarily indicate success, potentially reflecting a low negative predictive value in patients with prolonged ventilation and diaphragmatic dysfunction. This aligns with previous studies that showed decreased muscle strength despite an increased Tfdi [48]. Additionally, as there is currently no definitive TFdi cut-off for diagnosing diaphragmatic dysfunction [5], Tfdi may not be used as a universal index for accurately capturing diaphragmatic efficiency. We hypothesize that in these patients, despite having Tfdi values above 30–35%, diaphragmatic inflammatory injury [48] impaired its ability to generate sufficient pressure; the latter may had an important impact in weaning outcome and may have caused a compensatory increase in extra-diaphragmatic muscle activity, as PTPes almost doubled during IRL. As such, in populations such as ours, TFdi may demonstrate greater variability and may not be as reliable in predicting breathing effort, as in other patient groups. Moreover, Tfdi values < 30–35% may be used as a cut-off for weaning failure. Under resistive load, Tfdi, which reflects primarily contractile shortening, may not increase despite higher contractile forces.
Although Dex and TFdi share many similar characteristics [3, 49] (such as the 2D visualization of a 3D structure, limited representation of the respiratory muscle apparatus, and interpatient variability) they differed in their relationship with breathing effort and weaning outcomes. This difference is also reflected in the weak correlation between the two measures [50]. Tfdi assesses diaphragmatic contractility and Dex diaphragmatic displacement and possibly lung volume change [51, 52]. Specifically, at tidal volumes below 50% of inspiratory capacity TFdi reflects active muscle thickening and remains unaffected by lung volume [17]. In patients who rely more on rib cage muscles for inspiration [36, 39], tidal volume may drive diaphragmatic excursion, even with minimal or no increase in TFdi. Our hypothesis is that these characteristics of the two variables, led to the different relationships with breathing effort and weaning outcome.
Previous studies have evaluated breathing mechanics and diaphragm function under IRL [37,38,39,40, 53,54,55]. However, in some of them the breathing pattern was prespecified [38, 53], or the enrolled population was exclusively healthy subjects [37,38,39,40, 53, 54] making comparisons difficult. In two studies [53, 54], where diaphragmatic kinetics were assessed via ultrasound during unloaded breathing and IRL, the reported results were results similar to ours, as both Dex and Tfdi increased under IRL. In our study, the Ti/Ttot increased, while the MIF decreased during IRL, aligning with previous findings [37, 38, 54, 55]. However, some differences exist between our results and those of prior studies. For instance, two studies [37, 54] reported an increase in Vt and a decrease in RR, whereas in patients with upper airway obstruction [55], both Vt and RR remained unchanged. In contrast, in patients breathing with an IRL similar to ours [40], Vt decreased.
In our study, Dex correlated significantly with Vt during spontaneous breathing while no significant correlation was found during IRL. Moreover, there was an increase in Dex despite a decrease in Vt during IRL. In the current literature, the strong correlations between Dex and Vt refer mainly on healthy subjects [51, 52] and to our knowledge, there are no data on the relationship between them during resistive breathing in similar populations to ours. However, in a previous study [53], where Vt was kept constant, upon application of the same IRL, Dex increased. Moreover, when bilateral anterolateral magnetic phrenic nerve stimulation is conducted, with the airway occluded Vt does not increase despite the diaphragmatic contraction and displacement [56]. A possible explanation for this uncoupling is that the resistance reduces thoracic amplification. This might seem to counter the argument of increased extra-diaphragmatic muscle activity. However, as shown in previous studies [39, 40] patients breathing against a resistive load exhibited a more elliptical thoracic shape and reduced anteroposterior diameter, as well as lower Vt [40], accompanied by an increased activity of extra-diaphragmatic muscles. Moreover, the resulting thoracic shape appeared to be independent of diaphragmatic activity and was instead influenced by the preferential activation of specific extra-diaphragmatic muscles, such as the parasternals and intercostals. Therefore, we believe that a reduced thoracic expansion might not necessarily indicate decreased extra-diaphragmatic muscle activity; rather, it may reflect an increased contribution of these muscles to the overall inspiratory effort, which aligns with our hypothesis regarding their role in this patient cohort. Another plausible explanation may be that Dex assesses diaphragm at a certain local point which may be dissociated from global lung volume change during the application of resistive load. Measurement of the extra-diaphragmatic muscles activity or, electrical impedance tomography could provide further insight in our findings.
In the present investigation, RSBI in weaning success patients, increased under IRL but it remained within normal limits (< 110 breaths/min/L), unlike in weaning failure patients. It is of note that some patients who failed weaning presented RSBI values below 110 breaths/min/L during spontaneous breathing, but RSBI increased significantly (p = 0.016) with the application of IRL. These findings may suggest that patients who are successfully weaned may have greater respiratory reserve, allowing them to tolerate resistive loading without a significant change in their breathing pattern.
To our knowledge, most studies evaluating the relationship between diaphragmatic ultrasound and breathing effort have been conducted in subjects under positive-pressure ventilation, which can confound diaphragmatic ultrasound measurements and alter their relationship with breathing effort [5, 6, 17, 22]. Additionally, diaphragmatic ultrasound exhibits high interpatient variability [49], and its correlation with breathing effort has been inconsistent across studies [10, 14,15,16,17,18,19]. To address these limitations, we conducted our study during an unassisted spontaneous breathing trial (SBT) to eliminate the confounding effects of positive-pressure ventilation on diaphragm mechanics. To mitigate interpatient variability and focus on the intrapatient relationship between diaphragmatic ultrasound measurements and breathing effort, we employed repeated measures correlation [33], a statistical method designed to assess within-patient associations. Furthermore, the effect of an IRL on breathing mechanics has been studied mainly on healthy subjects. The application of such protocol in critical care patients may be challenging in terms of patient cooperation and clinical stability which are required for valid measurements. Moreover, the idea of applying a restive load during weaning might be perceived by physicians as a challenge which may induce respiratory muscle fatigue. Our rationale was that an IRL for a brief time (1 min) even though it may increase the breathing effort, it may be similar -if not less in magnitude- with a MIP maneuver of 30 s duration and may simulate a clinical scenario of increased resistive load to the respiratory system.
Certain considerations should be taken into account when interpreting our results. The weaning failure rate in this study was high. Similar failure rates have been previously reported [1,


Comments (0)