In this secondary analysis of the INTUBE study, peri-intubation severe hypoxemia was more common in obese compared to non-obese patients. Obesity was independently associated with first-pass intubation failure while being an experienced operator in airway management was independently associated with first-pass intubation success. Videolaryngoscopy was associated with increased first-pass intubation success when applied in the obese population.
Although severe hypoxemia was more common in overweight to severely obese patients in univariable analysis, obesity itself was not an independent predictor of peri-intubation hypoxemia. Instead, first-pass intubation failure, baseline oxygenation status and patient’s position, were variables associated with this event.
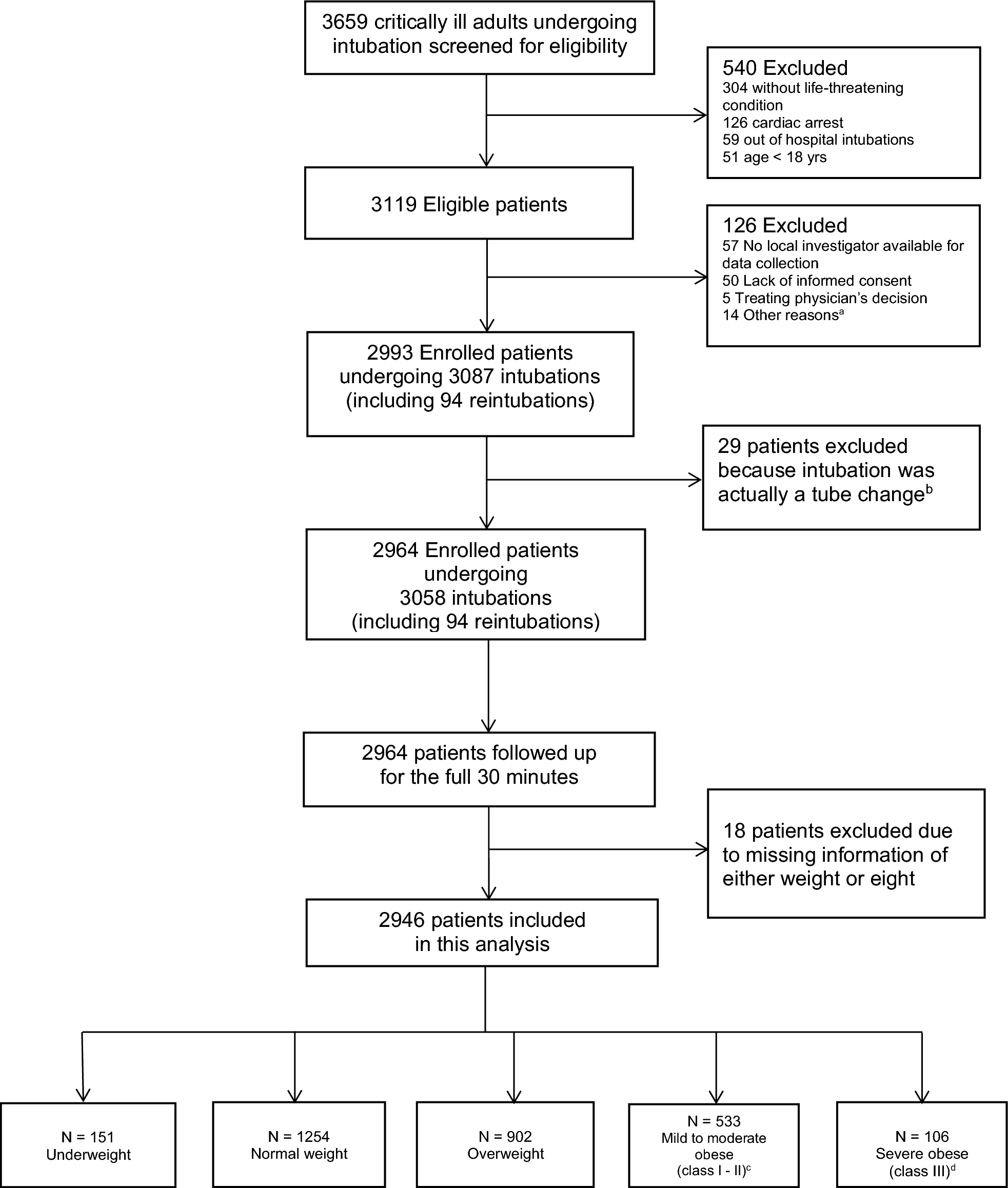
This study elucidates how a failed first intubation attempt exposes critically ill obese patients to a higher risk of developing severe desaturation during the procedure. This is an important finding, since obesity is a common condition in critical care, observed in 21.6% of patients in the INTUBE cohort, which is similar to the 20% of obesity observed in a French cohort [13].
In a multicenter French study, De Jong and colleagues investigated risk factors for difficult intubation (\(\ge\) 3 laryngoscopic attempts) along with developing and validating a specific prediction score for difficult intubation in ICU (MACOCHA score) [18]. Obese patients were at a significantly higher risk of difficult intubation in both developing and validation cohorts, but obesity was not included in the final model, which only included Mallampati score III and IV, reduced mobility of the cervical spine and limited mouth opening among patient’s specific variables [18]. Based on our data, the higher risk of first intubation attempt failure similarly seems to be driven by the higher frequency, in obese patients, of well-known predictors of difficult intubation, such as high Mallampati score, short neck and its increased stiffness, and reduced mouth opening. Indeed, each of these factors were independently associated with a higher first-pass intubation failure (Table S5 of the Supplementary Material).
Taken together, these findings may value once again the importance of obesity as an easily identifiable characteristic of a high-risk population for difficult airways in a daily clinical scenario of emergency intubation, as very likely summing up the presence of recognized anatomical predictors which, together with additional physiology features, define a potential difficult intubation. However, we should also highlight that obesity is a heterogeneous condition, as it comprises different typologies of adipose tissue distribution (i.e. central vs peripheral) with distinct pathophysiology and clinical implications [2]. We may argue that central obesity could exert more profound implications on respiratory physiology than peripheral obesity, and it could be more commonly associated with anatomical predictors of difficult airway management [3, 13]. In addition, our analyses were based on the widespread adoption of BMI, which represents an additional oversimplification of the complex obesity condition [19]. Accordingly, clinicians should anyway conduct a thorough airway assessment, incorporating individual anatomical and physiological risk factors, rather than relying solely on BMI as a surrogate marker of intubation difficulty [20].
Difficulty of manual ventilation in obese patients has not been investigated in this secondary analysis. This task may be crucial in case of first-pass intubation failure, when rescue oxygenation may be provided before a second attempt. Different anatomical features of obese patients (e.g., large tongue, short neck) may hamper effective mask seal or airway patency, and this has been reported in the anesthesia setting [9]. However, in our cohort most patients were intubated with a standard rapid sequence induction technique (i.e., no ventilation between induction and laryngoscopy) and information on difficult ventilation was therefore unavailable.
In this secondary analysis of INTUBE study, we focused on hypoxemia and first-pass intubation success since there might be an important interplay between these events during the peri-intubation period. Indeed, in clinical practice, the laryngoscopy attempt may be interrupted by intercurrent desaturation, in parallel with or irrespective from anatomy challenges [21].
In the anesthesia setting the benefit of ramp and different degrees of head-up positions have been documented, with an improvement of FRC and, consequently, of oxygenation as the primary mechanism [22]. In the critically ill setting, evidence on the benefit of patient’s position in terms of improved oxygenation and/or first pass success has been conflicting [23, 24]. We unexpectedly found an association of 30–45° head-up positioning with higher incidence of severe hypoxemia and 20° head-up positioning with greater first-pass intubation failure. Further research is warranted to determine if these associations reflect worse intubating conditions or patient selection characteristics.
Positive pressure ventilation, delivered either as NPPV or CPAP, was not associated with reduced peri-intubation hypoxemia in our cohort. This is in contrast with recent findings from a randomized trial showing the benefit of noninvasive ventilation compared to oxygen mask at preventing severe hypoxemia (SpO2 < 85%) in critically ill patients [25]. In this trial, severe hypoxemia occurred in 9.1% in the noninvasive ventilation group and in 18.5% in the oxygen mask group. In the sub-group analysis of this study including obese patients, authors showed an even higher benefit of noninvasive ventilation at preventing desaturation compared to oxygen mask [25].
We could argue that the lack of benefit of noninvasive ventilation in our cohort may be due to the presence of confounders, as inherent to the observational nature of the study. For example, more severe patients may have received positive pressure ventilation as ongoing noninvasive respiratory support, and this may have influenced its association with outcome. Of note, the use of positive pressure preoxygenation was not common in the overall population of our cohort (11.6%), and it was only slightly higher (15.5%) in the obese group. Our study was performed before the COVID-19 pandemic and current practice on preoxygenation may have been changed after this experience [26]. We should also point out that different interventions, whose effectiveness has been proved in randomized trials, are slowly implemented in real life clinical practice [27, 28].
Baseline oxygenation status was significantly associated with peri-intubation severe hypoxemia. A lower SpO2 before induction exposes patients to a higher risk of critical desaturation during the procedure, but it may also represent a marker of underlying disease severity (i.e., reduction of ventilated lung volume leading to increased pulmonary shunt and reduced oxygen reserve in the FRC) [29]. We should also highlight that ventilator settings, PEEP adjustments, and lung recruitment maneuvers play a critical role in preventing post-intubation hypoxemia, especially in obese patients who are highly prone to de-recruitment [8]. These variables were not collected in the INTUBE cohort, as we focused on airway management, but they should be considered for the interpretation of our results.
The MACOCHA Score highlights the utility of operator background in anesthesiology, again, confirmed in the present study [18]. De Jong et al. defined ‘anesthesiologist’ as a medical doctor with two or more years training in anesthesia. More work is necessary to define what constitutes adequate training in airway management in the critically ill adults [30, 31].
This analysis also emphasizes the need for the contemporary conceptual development of the Physiologically Difficult Airway as a paradigm for critical care airway management [32, 33].
Finally, our study confirmed the benefit of videolaryngoscopy to improve first-pass success in critically ill patients [34,35,36]. In our cohort, clinicians more frequently adopted videolaryngoscopy as first-choice device in obese patients and, in this population, it was associated with a twofold increase of first-pass intubation success.
The INTUBE study showed that the single most common life-threatening complication of airway management in critically ill adults was cardiovascular collapse [11, 37]. These data are reassuring in that obesity per se does not appear to worsen this outcome, despite concerns that patients living with obesity have a higher incidence of right ventricular strain [2, 3].
This study also speaks to wider patient safety considerations such as human factors and teamwork; senior clinicians should be awake to the risks posed by obese patients and manage the logistics and timing of intubation in this extremely vulnerable group accordingly [38].


Comments (0)