This case illustrates the rapid and devastating effects of AlP poisoning and underscores the difficulties in diagnosis when history from the patient is not forthcoming. The initial presentation of this patient with repeated vomiting, epigastric pain, and profound hypotension, in the absence of a clear toxicological history, presents a diagnostic challenge. His clinical deterioration, characterized by refractory hypotension, elevated cardiac enzymes, and metabolic derangements, was suggestive of severe systemic toxicity, though the source was initially unclear. This insidious course of disease progression, with the patient dying on the third day after presentation, also constituted a medical challenge due to the known rapid 24-hour mortality of AlP poisoning [3].
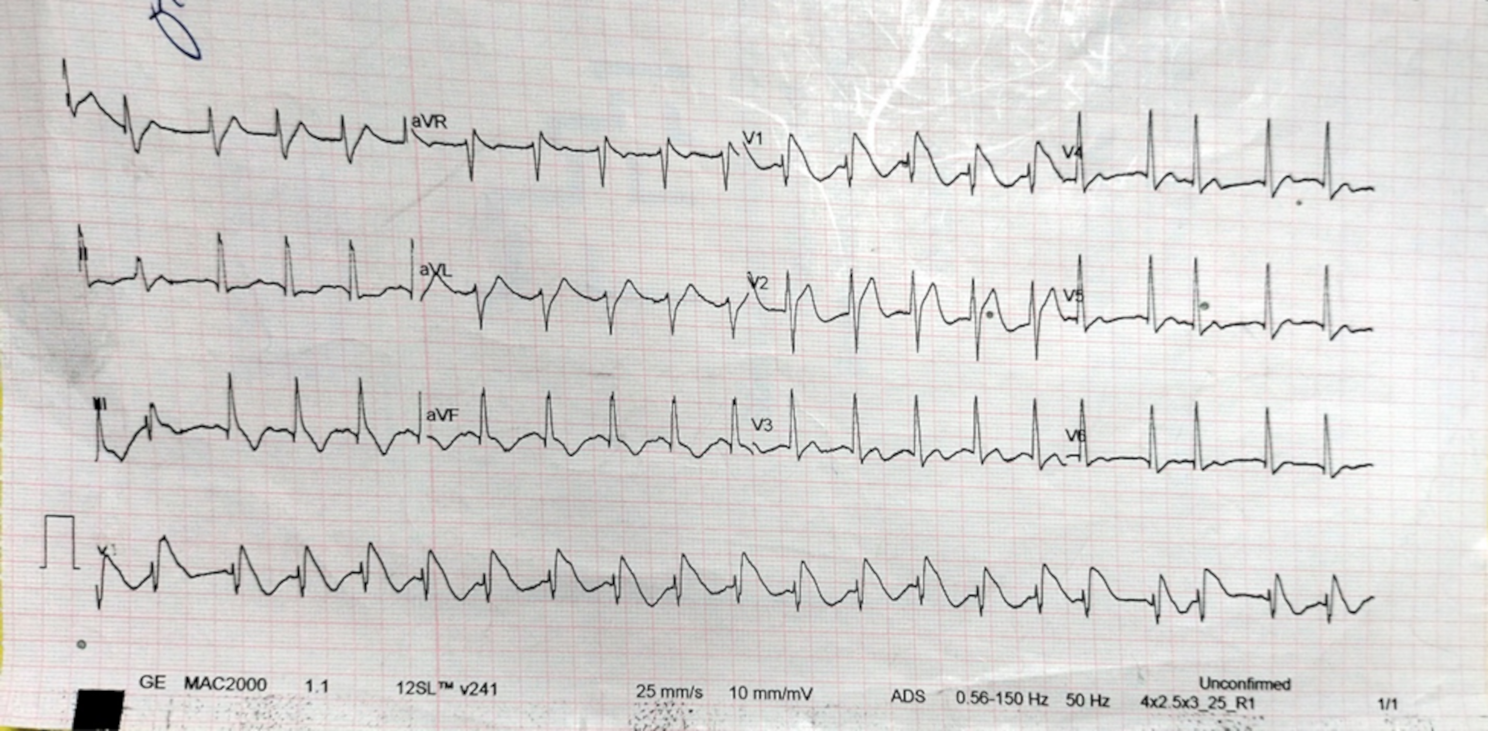
The ECG findings of coved ST-segment elevation in V1 and V2 with T wave inversions in V1-V3, while atypical, have been reported in cases of ALP poisoning and are often misinterpreted as signs of acute coronary syndrome [2, 4, 8, 11]. Elevated cardiac biomarkers in this case likely reflected direct myocardial damage due to phosphine gas rather than primary ischemia. Allam et al. [8] and Guru et al. [2] reported the occurrence of the Brugada pattern with AlP poisoning. However, they reported negative troponins in their case reports. AlP poisoning was also reported to be associated with STEMI with an ejection fraction of 15% in a 25-year-old man with no comorbidities [5]. Otherwise, published data on the association between cardiac arrhythmias and AlP poisoning was scarce and outdated [6, 7]. However, these outdated studies still reported the incidence of arrhythmias with AlP poisoning. For instance, Siwach et al. [6], have monitored the cardio-electrographic rhythms of 30 patients with AlP poisoning in 1998 and found that all patients had supraventricular and ventricular tachycardias, and as much as 40% of them had life-threatening ventricular tachycardia. However outdated, this warrants further investigation and might even warrant cardiac monitoring in patients with AlP poisoning.
Key laboratory findings in this patient, including elevated liver enzymes (ALT, AST), renal dysfunction (elevated creatinine), and coagulation abnormalities (prolonged PT, PTT, and INR), point to multi-organ involvement typical of ALP poisoning. Phosphine gas disrupts mitochondrial function, leading to widespread cellular damage, particularly affecting the heart, liver, and kidneys [12]. Additionally, the elevated serum amylase suggests possible pancreatic involvement, a less common but documented feature of ALP toxicity [13]. Moreover, the patient’s lab values showed significant hyperglycemia (240 mg/dl) before administration of D5W. A prospective cohort done by Mehrpour et al. reported that among 45 patients presenting with acute AlP poisoning, there was a statistically significant association between hyperglycemia (versus euglycemia) and mortality. However, there have also been reports of mortality associated with severe hypoglycemia [14, 15]. This underscores the importance of blood glucose monitoring and its importance in the prognostication of AlP poisoning.
The management of ALP poisoning is largely supportive, as there is no specific antidote. In this case, the patient was initially treated with aggressive fluid resuscitation and vasopressors to manage his profound hypotension. Unfortunately, his condition deteriorated despite these measures, which is a common outcome in ALP poisoning due to its high mortality rate. The administration of broad-spectrum antibiotics and proton pump inhibitors aimed to address possible secondary infections and prevent further gastrointestinal complications, though the primary pathology was driven by the toxic effects of phosphine gas. However, there has been a rising number of experimental clinical studies suggesting the use of magnesium sulfate, melatonin, N-acetylcystein, glutathione, sodium selenite, and vitamin C and E, among others, to reduce the hazardous oxidative properties of AlP [16,17,18]. Moreover, there have been reports of patients benefiting from extracorporeal membrane oxygenation (ECMO) in cases of acute AlP poisoning [19,20,21]. However, these treatments are still experimental and mostly inapplicable in the low-resource setting where AlP poisoning is prevalent.
This case highlights the importance of early recognition and intervention in suspected cases of ALP poisoning. However, the diagnostic process was delayed by the patient’s reluctance to admit to ingesting ALP, which is a common scenario in toxicology cases, particularly when patients fear legal or familial repercussions. The reluctance to disclose toxic ingestion emphasizes the need for a thorough and nonjudgmental history-taking approach, as well as a high index of suspicion in cases of unexplained shock, metabolic acidosis, and organ failure. Moreover, the diagnosis of this case was hindered but the insidious progression of the case, which in hindsight, could have been attributed to the expired AlP pellet. Despite the best efforts, the prognosis for patients with ALP poisoning remains poor, particularly in cases with delayed presentation or lack of early intervention. The patient’s progression to cardiac arrest despite aggressive treatment demonstrates the difficulty of reversing the toxic effects once multi-organ dysfunction has set in. Phosphine-induced cardiotoxicity and the refractory shock seen in this case are particularly resistant to treatment, often leading to fatal outcomes. Clinicians, especially in rural or low-resource settings, should maintain a high suspicion for AlP poisoning in patients with unexplained shock, metabolic acidosis, or Brugada-like ECG changes. Early supportive care, cardiac and glucose monitoring, and empathetic, nonjudgmental history-taking are essential to improve diagnosis and outcomes.
In conclusion, ALP poisoning remains a critical challenge in toxicology, particularly in areas where access to the substance is widespread. Early diagnosis and supportive care are crucial, but outcomes are often grim, as seen in this case. This case underscores the need for heightened awareness of AlP poisoning, particularly in patients presenting with unexplained gastrointestinal symptoms and shock, and highlights the importance of timely disclosure of toxic exposures to optimize management and improve prognosis, and the importance of glucose monitoring in prognostication of AlP poisoning patients. Furthermore, this case underscores the importance of increasing the medical suspicion regarding toxicological etiology, especially AlP poisoning, among acutely ill patients living in rural areas presenting with incomplete or vague history. Finally, the presentation of Brugada ECG in patients with the aforementioned presentation and vague history should also hint to AlP poisoning when no other medical diagnoses fit.






Comments (0)