
Remember me
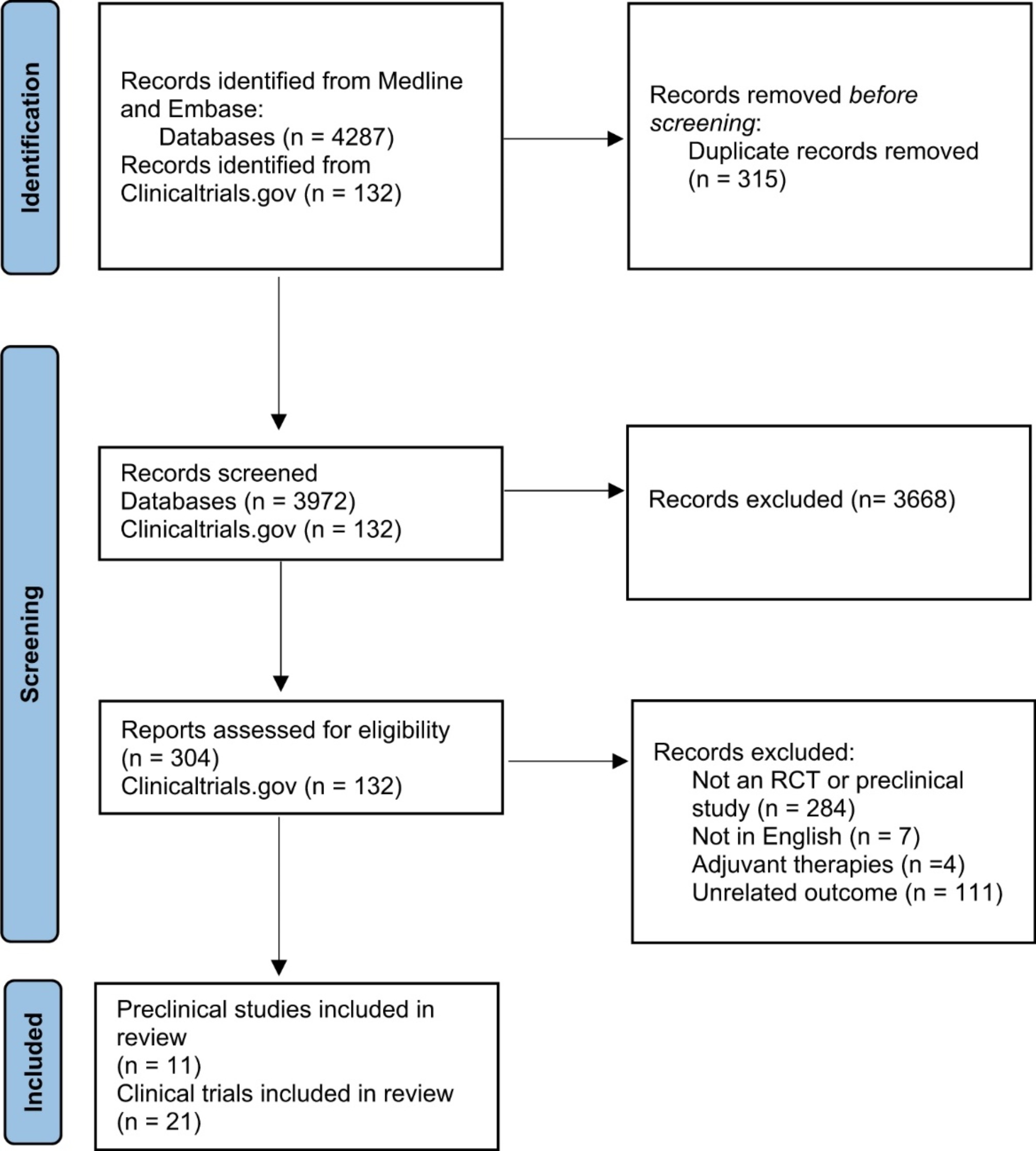





We searched Medline, Embase, and ClinicalTrials.gov databases, identifying a total of 4419 studies (4287 from Medline and Embase, and 132 from ClinicalTrials.gov). After removing duplicates, 4104 articles were screened by title and abstract, resulting in 436 potentially relevant studies. Following full-text screening, 32 studies met our inclusion criteria, including 21 clinical trials and 11 preclinical studies. Refer to Fig. 1 for a detailed description (Fig. 1). This study was also registered in PROSPERO under the number CRD42025640270. A title and abstract screening was performed according to PRISMA standards (the link below): https://www.crd.york.ac.uk/PROSPERO/view/CRD42025640270.
Fig. 1
PRISMA Flow diagram
Abbreviations: RCT: Randomized Clinical Trial
Pre-Clinical studiesDementia represents the foremost etiology of disability among individuals aged over 65 years, with its prevalence steadily increasing. Current therapeutic options fail to address key symptoms like psychomotor agitation, aggression, depression, and reduced physical activity [15]. Behavioral and psychological symptoms afflict at least 90% of dementia patients [15]. Given the absence of definitive pharmacological interventions, elucidating disease pathophysiology and exploring novel therapeutic agents are paramount. Animal models serve as indispensable tools in these endeavors [16]. Continued refinement of these models through ongoing research promises to bridge the translational dearth between preclinical findings and clinical applications [16].
Effective animal models must rigorously replicate human disease mechanisms to facilitate the development of efficacious treatments. Small animal models, such as mice and rats, offer distinct advantages including cost-effectiveness, reproducibility, and suitability for investigating related human pathophysiology and therapeutic pathways [17]. Animal models of AD encompass spontaneous, interventional, and genetically modified varieties [16]. However, while spontaneous models hold appeal, they pose challenges comprising the risk of zoonoses, maintenance costs, and variability in reproducibility due to extended lifespans [16].
Advances in genetic manipulation have facilitated the development of transgenic animal models that exhibit characteristics akin to AD, particularly in mice, preferred for their ease of genetic modification and shorter lifespans [16]. Rats, with physiological similarities closer to humans, offer advantages in studying motor behaviors but are hindered by technical limitations in genetic engineering [16]. For appropriate interpretation of study results, the influence of the genetic background on transgenic phenotypes must be carefully considered [16].
Animal models not only deepen our understanding of disease pathophysiology but also serve as essential tools for preclinical validation of potential therapeutic interventions [18]. Over the past two decades, substantial progress has been made in refining animal models for dementia research and evaluating therapeutic candidates [19].
Table 1 Overview of preclinical studies on stem cell therapy for dementia in Transgenic mouse modelsTable 1 summarizes the outcomes of preclinical studies utilizing various SCT for the management of dementia in transgenic mouse models [20,21,22,23,24]. The table categorizes SCT based on different cell classes, including Human PD-MSCs, Human U-MSCs, and others, each tested in specific transgenic models, that of B6C3-Tg (APPswe/PSEN1dE9) and Tg2576 (APPswe). Injection types varied, encompassing intravenous and stereotactic approaches, tailored to target affected brain regions effectively.
Outcomes observed across studies predominantly focused on improvements in spatial memory, assessed through tasks like the Morris water maze and novel object recognition tests. Additionally, reductions in inflammatory markers such as interleukins (ILs) and tumor necrosis factor (TNF) were reported, indicating potential neuroprotective effects. Mechanistic insights highlighted included neurotrophic support, modulation of microglial responses, and protection against amyloid-beta (Aβ) neurotoxicity, underscoring the multifaceted approaches of SCT in mitigating dementia-related pathologies.
Table 2 Comprehensive analysis of stem cell therapy outcomes in dementia treatment: Transgenic mouse models and stem cell typesTable 2 presents a detailed overview of SCT outcomes in dementia therapeutics, specifically focusing on diverse transgenic mouse models and their responses to various SC types [25,26,27,28,29,30]. The table categorizes SCT based on cell classes such as Human PD-MSCs, Human U-MSCs, and others, each evaluated in models including Aβ1–42-infused and specific transgenic strains like that of B6C3-Tg (APPswe/PSEN1dE9) and Tg2576 (APPswe).
Injection methods varied and included intravenous and stereotactic administration, both tailored to optimize therapeutic delivery and efficacy in experimental contexts. Reported outcomes predominantly highlighted improvements in spatial memory performance, often assessed using the Morris water maze test. Additionally, reductions in pro-inflammatory cytokines such as IL-1β and TNF-α, coupled with increases in anti-inflammatory cytokines like IL-4 and IL-10, underscored the immunomodulatory effects of SCT in mitigating neuroinflammation.
Mechanistic insights elucidated included neurogenesis support, modulation of microglial immune responses, and protection against Aβ-induced neurotoxicity, emphasizing the diverse therapeutic mechanisms employed by SCT in combating dementia pathology.
Clinical studies involving stem cell therapy in dementia casesSeveral clinical trials investigating SCTs for dementia are currently at different stages. Our review identified 21 trials, of which 6 have been completed, with results available for 4. Six trials are actively recruiting or awaiting initiation, while the statuses of 6 trials were undisclosed, 2 trials withdrawn, and 1 trial no longer available. Most trials examined employed human MSCs delivered via intravenous, intracerebral, and intraventricular routes, with intranasal administration also under exploration for its potential benefits. Table 3 summarizes these trials, detailing their recruitment status, phase, cell type, route of administration, and key findings.
Table 3 Status and findings of clinical trials on stem cell therapy in dementiaAmong the completed trials, NCT01297218 investigated the employment of human UCB-MSCs administered via intracerebral infusion [30]. The study reported acute adverse events in all nine subjects during a 12-week follow-up period, with no serious adverse events observed over a 24-month follow-up. Importantly, no dose-limiting toxicities were reported, highlighting the safety profile of this approach [30]. In contrast, the trial registered under NCT02054208 [31], which utilized human UCB-MSCs administered via intraventricular infusion, reported acute adverse events within 36 h of administration. The most common adverse events included fever (n = 9), headache (n = 7), nausea (n = 5), and vomiting (n = 4), all of which resolved spontaneously within 36 h. Serious adverse events were observed in three participants; however, no dose-limiting toxicities were reported [31].
Several ongoing trials are exploring different SCT approaches. For instance, NCT03724136 is currently recruiting participants to investigate the use of BM-MSCs administered via intravenous fractionation, with results yet to be published [32]. Similarly, NCT04388982 aims to evaluate the efficacy of MSC-derived exosomes administered via nasal drip, with results pending publication [33]. A notable withdrawal due to the novel coronavirus disease 2019 (COVID-19) pandemic is documented in NCT04228666, which planned to investigate the application of Hope Biosciences’ autologous A-MSCs via intravenous infusion [34]. The trial was halted without published findings [34]. Moreover, trials such as NCT03117738, utilizing autologous A-MSC via intravenous infusion, reported serious adverse events in three out of eleven subjects, underscoring the importance of rigorous safety monitoring in SCT trials [35].
In summary, although a number of clinical trials have shown encouraging results about the safety and possible effectiveness of SCT in the management of dementia, variability in outcomes and difficulties like adverse events require ongoing research and standardized methodologies to advance SCT as a viable therapeutic option.
Pre-clinical studies have extensively assessed the safety and efficacy of SCT using murine models, yet translating these findings into clinical trials has been limited. This discrepancy stems from the complex ethical considerations and uncertainties circumventing the safety of stem cell transplantation in human subjects. Globally, regulatory frameworks and policy interventions govern the funding and conduct of human clinical trials involving SCT [36, 37]. Selecting the appropriate cell source and type is crucial for enhancing the success of SCT. Notably, MSCs are favored in clinical trials targeting neurodegenerative diseases due to their ability to differentiate into non-hematopoietic stromal and neural cell lines, alongside their low immunogenicity [38, 39].
Table 4 Diverse types of stem cells utilized in human clinical trials for neurodegenerative disorders [40]Table 4 provides a comprehensive overview of various SC types investigated in human clinical trials for neurodegenerative disorders [40]. Pluripotent stem cells (PSCs), such as that of human-induced embryonic stem cells (hiESCs) and hiPSCs, offer potential for cell-replacement therapy and modeling neurodegenerative diseases in vitro [40]. However, challenges include phenotype instability and ethical controversy which hinder their widespread application [40]. Multipotent stem cells like that of NSCs and neural crest stem cells (NCSCs) present advantages such as neuroregenerative capabilities without the need for immunosuppressants, yet they face limitations in differentiation potential and self-renewal capacity. Additionally, MSCs derived from bone marrow and the blood of the umbilical cord are extensively studied for their anti-inflammatory properties and potential in tissue repair [40]. Nevertheless, optimal dosing and administration routes remain unresolved issues due to several factors [40]. The optimal dosing and routes of administration for mesenchymal stem cells (MSCs) remain unresolved due to several factors. MSCs derived from different sources (e.g., bone marrow, adipose tissue) exhibit variability in properties, making standardization difficult [40]. Additionally, the survival and distribution of MSCs vary depending on the delivery route, such as intravenous or intracerebral injection, with systemic delivery often resulting in low cell homing to the target site [40]. The dynamic inflammatory environment post-injury further complicates timing and effectiveness. Moreover, the lack of large-scale clinical trials with standardized protocols hinders the establishment of evidence-based guidelines [40]. These findings highlight the diverse landscape of SC types under investigation, each presenting unique advantages and challenges in advancing neuroregenerative therapies.
Quality assessmentAll 32 articles collected were thoroughly analyzed for adherence to the research question.
Various types of stem cells were investigated across clinical and preclinical studies:
BM-MSCs: Bone Marrow-Derived Mesenchymal Stem Cells.
iPSCs: Induced Pluripotent Stem Cells.
NSCs: Neural Stem Cells.
PD-MSCs: Placenta-Derived Mesenchymal Stem Cells.
U-MSCs: Umbilical Cord Warton’s Jelly-Derived Mesenchymal Stem Cells.
U-MSC-NCs: Neuron-like Cells differentiated from Umbilical Cord Warton’s Jelly-Derived Mesenchymal Stem Cells.
UCB-MSCs: Umbilical Cord Blood-Derived Mesenchymal Stem Cells.
MSCs-Exos: Exosomes from Allogenic Adipose Mesenchymal Stem Cells.
HB-adMSCs: Hope Biosciences Autologous Mesenchymal Stem Cells.
AD-MSCs: Adipose-Derived Mesenchymal Stem Cells.
LMSCs: Longeveron Mesenchymal Stem Cells.
AD-SVF: Autologous Adipose-Derived Stromal Vascular Fraction.
The age of recruited subjects for the trials was unspecified in the literature and thus not included in the review.
Stem cells were administered via various routes:
Bilateral intra-hippocampal stereotactic injection.
Bilateral intraventricular stereotactic injection.
Intravenous infusion.
Intracerebral infusion.
Intraventricular infusion.
Intranasal infusion.
The duration of administration was not specified in the reviewed works.
Methods used to evaluate outcomes in stem cell trials included:
Donor cell migration and differentiation.
Spatial memory.
Levels of phosphorylated tau proteins and amyloid β-plaques.
Expression of pro-inflammatory cytokines.
Levels of neural microglia.
Severity of adverse events.
Dose-limiting toxicity.
The number of animals implicated for stem cell transplantation was not specified in the review.
Comments (0)