Study design and patient population
A single-center retrospective analysis was conducted of 97 pediatric patients (49 males, 48 females) with de novo AML treated at St. Anna Children’s Hospital, Austria, between October 1998 and January 2023. Overall, 92 patients (95%) received at least one AFP cycle with AmB, itraconazole, or voriconazole. Eligibility required an AML diagnosis treated under the AML-BFM protocols [11, 12]. Exclusions included patients receiving no AFP (n = 3), alternative AFP (n = 1), or those with a prior history of IFD (n = 1).
Local protocols for AFP were continually adapted to reflect emerging options. AmB was the primary prophylactic agent until 2004, when liposomal AmB (L-AmB), itraconazole, and voriconazole became available. Itraconazole use ceased due to poor bioavailability and limited availability of oral solutions. Since 2018, L‑AmB and voriconazole have been primarily used. Patient treatment occurred in one of two oncological wards, where a specific protocol was followed: One ward adopted novel supportive treatments, while the other adhered to established practices, in the case that two prophylactic regimens were available simultaneously. The allocation of antifungal drugs was based on the admitting ward, ensuring equitable treatment across two wards.
Parental or patient informed consent for data registration and follow-up was obtained in accordance with local laws and regulations. This retrospective study was conducted in line with the Declaration of Helsinki and was approved by the Ethics Committee of the Medical University of Vienna, Austria (EK Nr.: 1761/2017).
Assessment of antifungal prophylaxis
Antifungal prophylaxis was initiated after chemotherapy at the onset of severe neutropenia (absolute neutrophil count [ANC] ≤ 0.5 g/L) and continued until neutrophil recovery or the next chemotherapy course.
AmB was administered at 1 mg/kg/day and L‑AmB at 3 mg/kg/day, both intravenously on alternate days. Itraconazole was administered at 5 mg/kg/day and voriconazole at 4–8 mg/kg twice a day with a maximum daily dosage of 400 mg, both orally. Therapeutic drug monitoring for azoles was inconsistently performed due to limited availability and therefore not evaluated in this study.
Assessment of safety and tolerability
The study focused on agent-specific adverse events (AEs) reported in the literature. The observation period for AEs was defined as the time from AFP initiation until the next chemotherapy cycle, the switch to another agent, or the start of antifungal treatment. The observation period was restricted to intensive chemotherapy only.
Clinical and laboratory AEs were graded according to the US National Cancer Institute’s Common Terminology Criteria for Adverse Events (CTCAE v 5.0). Infusion-related reactions were recorded but not graded.
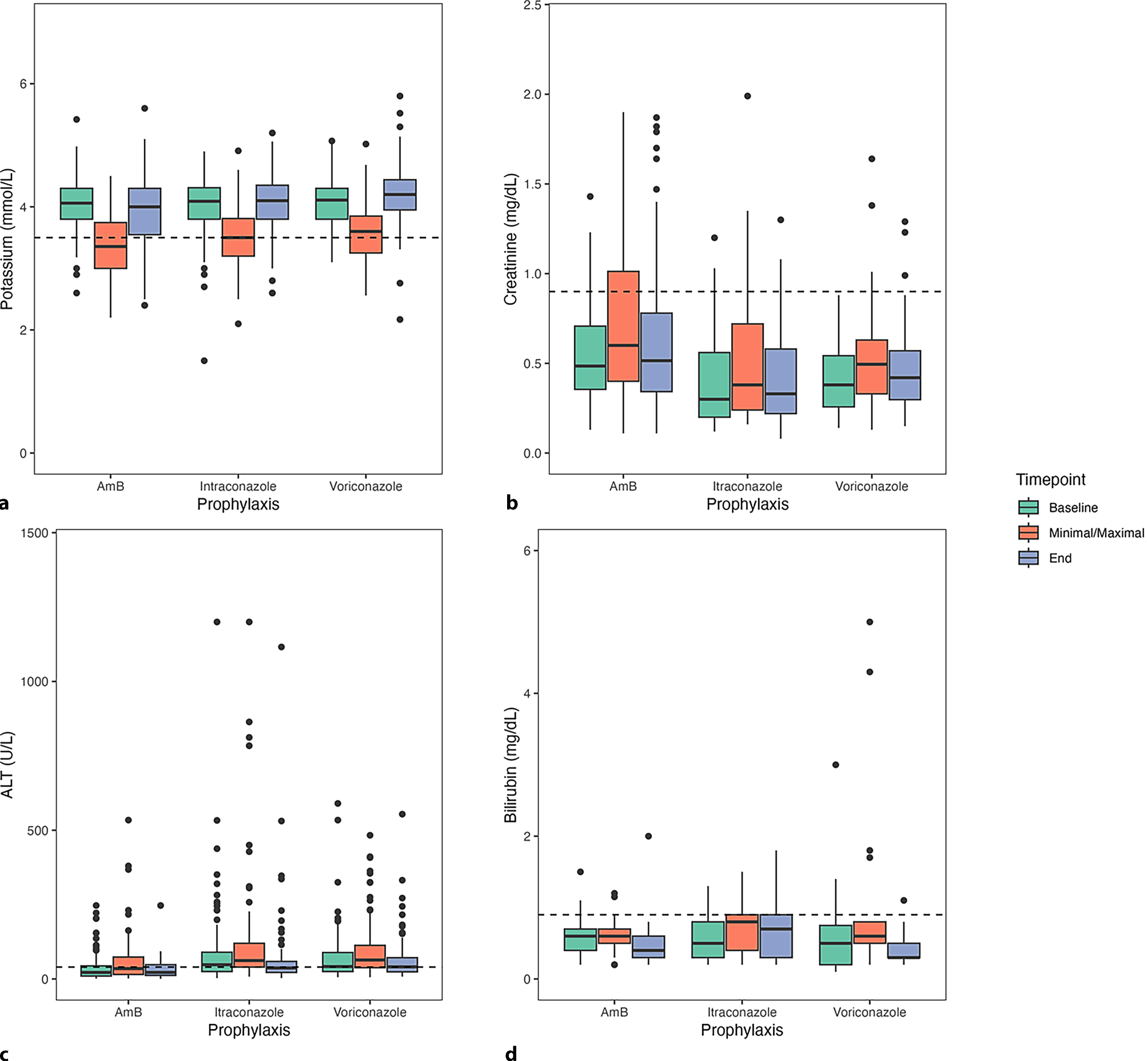
Renal toxicity, assessed through serum potassium and creatinine levels, and hepatotoxicity, evaluated using ALT and total bilirubin levels, were documented. Electrocardiograms (ECGs) for the evaluation of QTc prolongation were not routinely performed initially but were later conducted prior to the start of the next chemotherapy course or in response to clinical abnormalities, with patients still receiving AFP at these times.
Assessment of efficacy
Successful AFP was defined as the absence of treatment switches or discontinuation due to AEs. All patients under prophylaxis were monitored for clinical, laboratory, or radiological changes indicative of IFD.
Diagnostic measures were initiated according to pediatric guidelines for patients with persistent febrile neutropenia (fever ≥ 38.0 °C for 1 h or a single temperature ≥ 38.5 °C) combined with low neutrophil counts (ANC ≤ 0.5 g/L), unresponsive to broad-spectrum antibiotics after 96 h, or showing any clinical sign consistent with IFD. The diagnostic workup included chest radiographs, high-resolution computed tomography scans, and magnetic resonance imaging of cranial and sinus regions to exclude CNS and sinus involvement [5, 13]. There was no standardized policy on the use of biomarkers during the early phase of the study due to limited availability. However, with the introduction of broad-spectrum fungal PCR and galactomannan tests, these methods were incorporated into routine diagnostic procedures. Whenever possible, samples for culture and histology were collected from suspected infection sites. The diagnosis of invasive fungal infection was made based on international consensus criteria, classifying IFD as probable or proven [14, 15].
Empirical antifungal treatment, initiated at clinical suspicion of IFD, or preemptive antifungal therapy, guided by early biomarkers or imaging findings suggestive of IFD, were initiated according to standard guidelines [5, 6].
Supportive care
All patients received Pneumocystis jirovecii prophylaxis with trimethoprim-sulfamethoxazole three times per week, oral non-absorbable AmB for candida prophylaxis, and paromomycin for enteral decontamination until the end of consolidation.
The use of antibacterial prophylaxis was initially inconsistent. From 2015 onward, systemic antibiotic prophylaxis targeting viridans-group streptococci was administered to patients during neutropenia [16]. As part of standard supportive measures, patients were nursed in single rooms, provided with a low-bacterial diet, and placed in protective isolation with high-efficiency particulate air filtration during phases of profound neutropenia.
Statistical analysis
Descriptive data are presented as percentages for categorical variables and as means with standard deviations (SD) and interquartile ranges for continuous variables. All statistical analyses were conducted using R (R Core Team, 2023) [17]. A two-sided p value below 0.05 was considered statistically significant.




Comments (0)