Sarcoma of the spermatic cord is a very rare tumor accounting for less than 1% of sarcomas [1]. The most common age of presentation is predominantly between the 6th and 7th decades of life, and it rarely occurs before the age of 20 [1,2,3, 5, 8,9,10). Our patient presented at the age of 54 years. Low-grade myxoid fibrosarcoma presents mainly in the extremities, with a less common occurrence in the trunk and upper limbs; abdominal and retroperitoneal presentation is even less common and unheard of (1, 10,11,12,13).
To date, there are fewer than 30 cases of malignant myxofibrosarcoma of the spermatic cord, of which only 4 cases are low-grade variants [4, 9, 11, 14,15,16). These patients usually present with painless scrotal or inguinal swelling, which increases in size progressively, although some patients may experience some type of associated pain [1].
Myxofibrosarcoma is a notorious tumor with a high degree of recurrence and metastasis. Local recurrence in these groups of tumors may reach up to 50–60% regardless of the tumor grade, but metastasis is uncommon in low-grade tumors [1, 12, 13]. However, there are contradictory reports from Angervall L et al., with low-grade tumors (grades I and II) showing less recurrence than high-grade tumors (GRADE III and IV)[10]. A short interval of recurrence is associated with poor clinical outcomes[12]. However, up to 20–30% of intermediate- and high-grade varieties can metastasize, mainly to the lung and vertebrae [1, 12]. Metastasis was less likely when the tumor was small, superficially located, or had a prominent myxoid component [13]. Lymph node involvement, however, is very uncommon, and lymph node dissection is usually unnecessary [1].
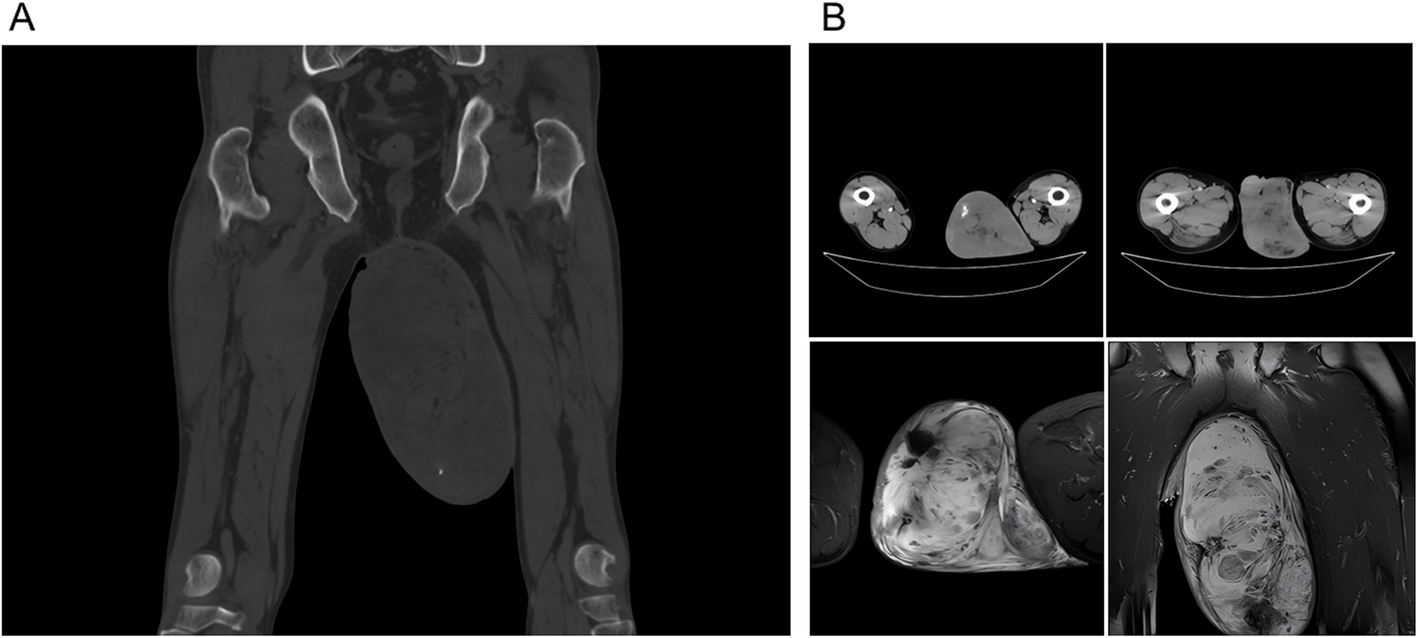
The diagnosis is made via ultrasonography, which reveals a para-testicular solid mass with areas of hyper-echogenicity, which is exactly what we have found in our patient. Imaging of the abdomen for retroperitoneal lymph nodes was normal. The final diagnosis is made on histopathological examination, which reveals proliferations of spindle cells with a collagenous and myxoid background admixed with tumor giant cells. IHC will differentiate it from similar mesenchymal tumor as it is positive for vimentin and negative for S-100 myogenin [2, 4].
Considering the relatively malignant nature of this mass and the possibility of local recurrence and distant metastasis, the main modality of treatment is radical surgery with negative soft tissue margins [1, 5, 9, 15). Those tumors with positive soft tissue margins have a high degree of recurrence and mortality, and additional treatment is warranted in this scenario [11]. In his case series of scrotal sarcoma, Unlü Y et al. reported that two of the patients with myxofibrosarcoma who had a positive margin died within 2 years after they refused adjuvant therapy [11]. In our case, we were able to achieve a negative gross margin of 9 cm, and the microscopic spermatic cord shave margin was also free. Considering the pathological stage, negative tumor margin and low-grade nature of the disease, adjuvant therapy was deferred, and strict follow-up due to the high risk of recurrence was selected for our patient.






Comments (0)