The clinical symptoms and physical examination findings of patients with scrotal AMF lack specificity, making a definitive diagnosis before surgery challenging, as shown in Table 1. Accurate diagnosis mainly relies on pathologic and immunohistochemistry findings and imaging can only be used as a reference [1,2,3,4, 6,7,8,9]. The morphology of scrotal AMF is specific with clear boundaries distinguishing scrotal AMF from surrounding tissues and a somewhat round shape [1, 4, 9], usually with a diameter < 5.0 cm. The largest reported diameter of scrotal AMF is 13 × 10 × 6 cm [9]. The current case reported a diameter of 25 × 15 cm in size, which is rarely reported. The patient lived in remote area in the mountains, and he had knowledge and little attention about his own health problems. That may be why the tumor grew to so big until he came to hospital for treatment. However, AMF occurring in women may be larger. In fact, the largest AMF report in women is 34 cm [10].
The tumor is elastic and soft, spongy or mucinous, and white or yellow–brown in color but lacks a fibrous or pseudo-coated surface and does not undergo hemorrhage or necrosis. Microscopically, the tumor is enriched with thin-walled blood vessels and scattered myofibroblasts, most of which are aggregated around the vessels in sparse and dense distributions [11, 12]. The myofibroblasts are spindle-shaped or ovoid and slender or obese, with a moderate amount of slightly acidic cytoplasm. The nucleus is oval with fine chromatin and inconspicuous nucleoli, occasionally showing nuclear atypia. Some cells are ovoid, with eosinophilic translucent cytoplasm, resembling those in plasma cell–like salivary gland mixed tumors [11, 12]. The arrangement of tumor cells in sparsely cellular areas is consistent with the direction of collagen fibers [2, 7, 8]. The clinical features, histologic structure, and immunophenotype of the patient in this case report were consistent with the literature [2, 7, 8, 11, 12].
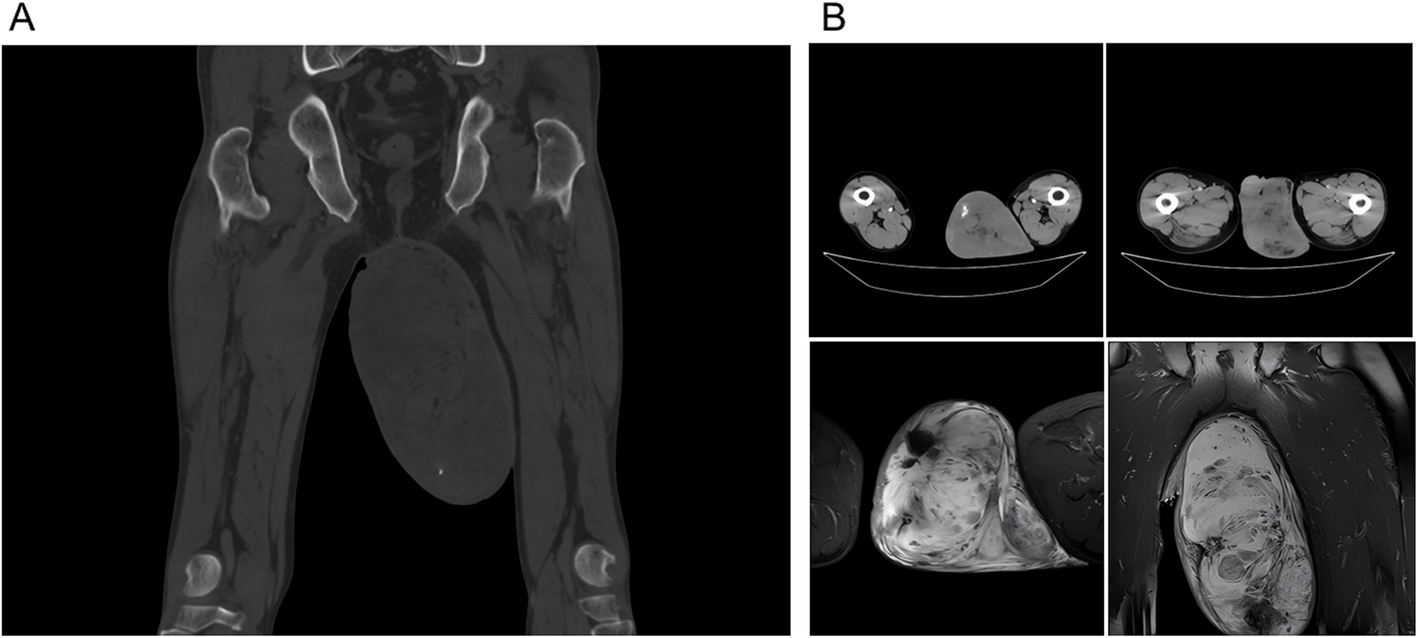
MRI, CT, and ultrasound are often used to helped diagnose scrotal AMF in clinical practice. The current case report showed that an abnormal signal in the scrotum in size of 12.6 cm * 9.4 cm with a clear boundary under MRI of the left scrotum [1, 4, 9]. Previous reports showed that germ cell tumors under MRI showed multiple nodules, and the number of fibrous and vascular compartments varied, and the thickness was uneven [13]. The images and clinical differences were summarized in Table 2, which should be focused in clinical practice [1,2,3,4,5,6,7,8,9, 13]. AMF is often benign [1,2,3,4,5,6,7,8,9], and germ cell tumor is often malignant [13]. However, the accurate diagnosis of scrotal AMF still need the pathological findings to support.
Table 2 The CT differences between AMF and germ cell tumorsWhen combined with pathologic findings, an AMF diagnosis can be established [1,2,3,4,5,6,7,8,9]. The most important clinical implication for urologic practice is the avoidance of overtreatment. AMF is a benign tumor, and correct diagnosis avoids unnecessary orchiectomy or radical surgery. Surgical treatment is the optimal choice when an abnormal mass is confirmed in the scrotum [1,2,3,4,5,6,7,8,9]. However, negative tumor markers are not consistent with a lesion. This situation highlights the difficulty in diagnosing scrotal AMF. Therefore, further in-depth studies with a focus on the pathogenesis of AMF and optimal therapeutic strategies are needed. Because of the low prevalence of scrotal AMF, multicenter collaboration involving imaging, urology, and pathology departments will help distinguish AMF and enable the patient to undergo treatment as early as possible. For the initial evaluation and management of patients presenting with scrotal masses of unknown cause, exhaustive specialty workup is paramount, and AFP CT MRI remains an important adjunctive test for identifying AMF, germ cell tumors, and intraoperative re-examination is critical to avoid misdiagnosis and misdiagnosis. As the age of AI approaches, AI-assisted image analysis of such research areas is particularly critical to improving our understanding of scrotal AMF. To achieve better therapeutic outcomes, treatment strategies for AMF should be based on rigorous imaging evaluation and pathologic analysis, as well as the clinical characteristics and individual differences.
No reports exist of patients with recurrent or advanced disease [1,2,3,4,5,6,7,8,9, 11, 12]. The patient in this case report recovered fully. Further follow-up with this case report is needed.
Scrotal AMF is a rare tumor that has an oval shape in the scrotum the size of a chicken egg. Patients often feel the mass but are asymptomatic. Imaging, pathologic findings, and tumor biomarkers can help diagnose and treat the patient. Surgery is the optimal option for patients and no recurrences have been reported in patients with scrotal AMF. However, due to the low incidence of AMF, few in-depth studies have been conducted. Research on scrotal AMF is still in the early stage and further exploration of the etiology, pathogenesis, and therapeutic strategies is needed.






Comments (0)