
Remember me


The current study is a double-blind randomized controlled trial (RCT) with six conditions (MBT, CCT, and ABT vs. sham MBT, active-sham Peripheral Vision Task (PVT) and sham ABT) with an observational one-year follow-up, conducted at Radboud university medical centre, Nijmegen, the Netherlands. After obtaining approval for the study from the Medical Ethics Committee Arnhem-Nijmegen (NL60033.091.16/2016–3009), recruitment started in January 2019. The study is registered at the Overview of Medical Research in the Netherlands (NL-OMON26184 and NL-OMON27513). See Supplementary Material for summary of trial registration data.
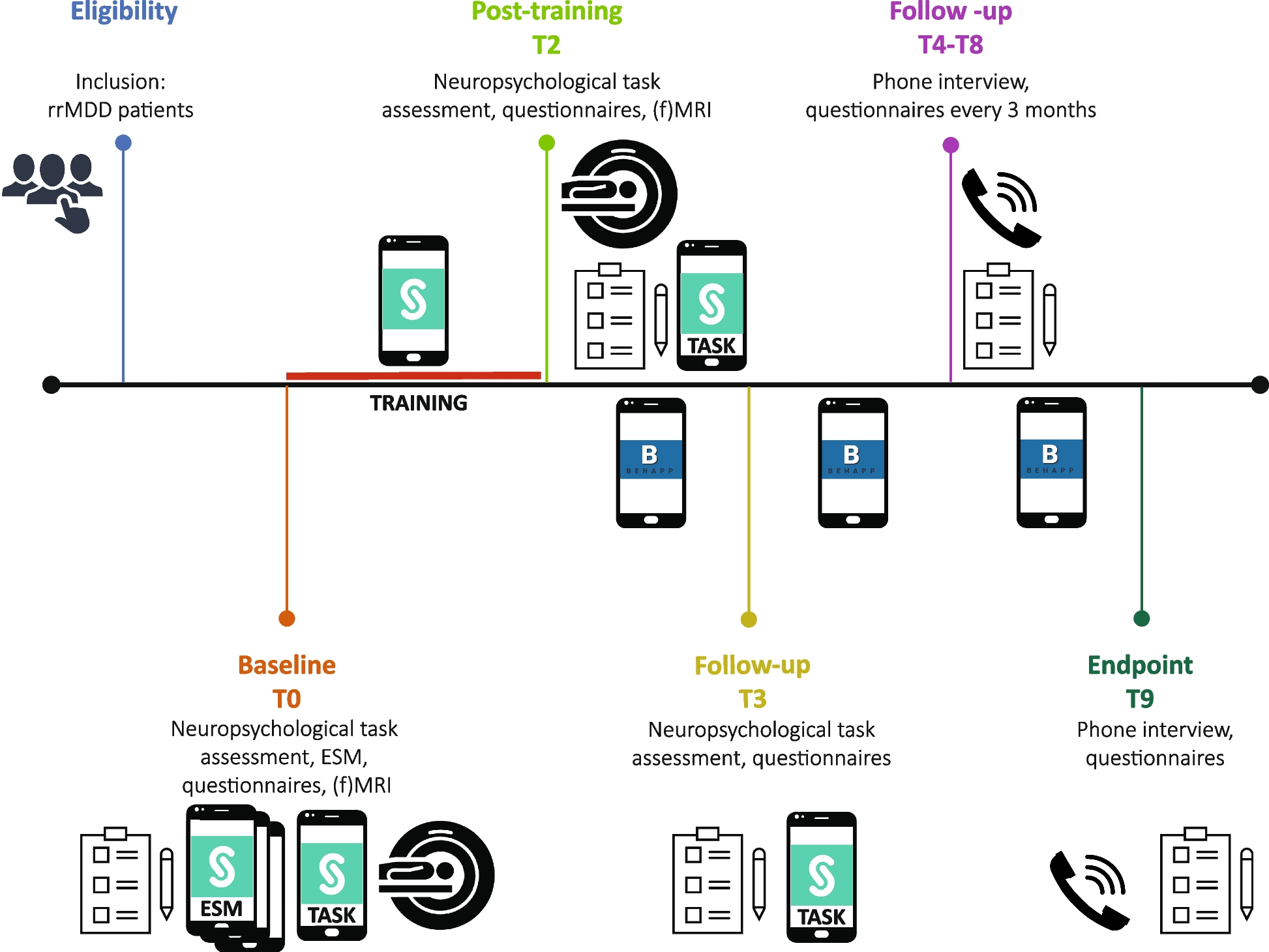
In brief, remitted MDD-patients with recurrent-MDD will complete baseline cognitive tasks on their smartphone, pre- and post-training. Then, they will receive one or multiple training sessions per day (depending on condition, described below) on their smartphone, over the course of three weeks. MRI-eligible participants will be invited to the research site to acquire a pre- and post-training MRI-scan. Four weeks after the end of the training period, participants again complete cognitive tasks on their smartphone. During a subsequent one-year follow-up, participants will be called every three months to assess recurrence-status of depression (using the Structured Clinical Interview for Axis I Disorders; SCID-I [83]. See Fig. 1 for an overview of the recruitment and design. Substantial amendments to the research protocol will be addressed to all relevant parties (i.e., medical ethics committee, trial register, journals). The reporting of this manuscript is in compliance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines.
Fig.1
Design of the Smartphone-based Monitoring and cognition Modification Against Recurrence of Depression (SMARD) study. Assessment time-points of the study are shown in chronological order from left to right. For a description of the questionnaires please see Supplementary Material
Recruitment of participantsParticipants will be recruited via advertisements in newspapers, common website and forums for depression. Interested participants can easily contact the researchers. Moreover, individuals with known MDD in remission can be referred by health care professionals in primary care (e.g., general practitioners) and/or mental healthcare organizations. In addition, we will send information letters to potentially eligible patients with recurrent MDD identified from previous studies, electronic medical records in our outpatient departments, and general practitioners. Interested individuals will be informed with written information about the study and contacted by telephone to elucidate this information within a week.
In- and exclusion criteria for participantsInclusion criteriaIn order to be eligible to participate in this study, an individual must meet all of the following criteria:
Recurrent MDD diagnoses and at least three previous MDD-episodes assessed by a SCID-I;
Not fulfilling criteria for a current active MDD episode (based on the SCID-I);
Score ≤ 10 on the Hamilton Depression Rating Scale (HDRS [84]);
Being in stable remission (≥ 8 weeks)
Age 18–65 years;
In possession of a smartphoneFootnote 2 and experienced in the use thereof.
Exclusion criteriaIndividuals who meet any of the following criteria will be excluded from participation in this study:
Diagnosis of bipolar, primary psychotic or borderline/antisocial personality disorder or strong suspicion of this type of disorder;
Primary diagnosis of substance use or anxiety disorder with secondary MDD (comorbid secondary anxiety disorders are allowed for participation);
Electroconvulsive therapy (ECT) within two months before inclusion;
Average alcohol intake of > 3 units/day;
Daily use of benzodiazepines (≥ 5 mg diazepam or equivalent).
Additional general exclusion criteriaOngoing psychotherapy during the cognitive training;
Previous CCT, MBT or ABT training.
Additional MRI exclusion criteriaFor the MRI-part of this study, standard MRI exclusion criteria will apply:
Metal objects in the body;
Claustrophobia;
A history of head trauma or neurological disease, severe general physical illness.
If a participant uses more than one smartphone, they will be requested to complete the assessments and cognitive training on the smartphone used for private matters. Participants with ongoing use of antidepressants are allowed to participate. For neuroimaging no exclusions will be based on handedness.
Randomization and blindingBefore the start of the cognitive training, participants are randomized by one of the investigators (HGR or AT; not involved in diagnostic follow-ups) to receive either true MBT, sham MBT, true CCT (Paced Auditory Serial Addition Task; PASAT [85]), active-sham CCT (PVT), true (positively skewed) ABT or sham (equally distributed) ABT. Randomization will be stratified for use of antidepressants (i.e., yes or no) and residual depressive complaints (i.e., HDRS > 5 vs. HDRS ≤ 5). Concealment of randomization is secured by using the randomization program of Castor EDC, a cloud-based Electronic Data Capture platform, to safely collect, integrate and manage data. True vs. (active-) sham condition will be fully blinded for the MBT, CCT, and ABT, for both participants and clinical assessors. Randomization is managed by a researcher not involved in the assessments.
In order to compensate for withdrawal from the study all participants with insufficient cognitive training (< 80% of completed sessions) will be replaced. In order to obtain adequate groups for neuroimaging, ≥ 20 participants per true or (active-) sham condition will be recruited with useable pre and post-training MRI data; therefore quality of MRI data will be checked shortly after acquisition.
Randomized trainingMemory Bias Modification Training (MBT) versus sham MBTIn the true MBT and sham MBT, eight prompts will be given per day for a period of 21 days. All prompts will be delivered in semi-random intervals between 06.30 and 23.30 h, tailored to the individual’s normal routine of waking up and going to bed. Completion of a prompt takes approximately 3 min.
Every day, participants will receive a prompt at the start of the day with a sleep-related question (“I slept well) with answer options on a 7-point scale ranging from ‘not at all’ to ‘very well’. At each prompt the participant will be asked to assess his/her current mood using statements regarding positive mood, negative mood, relaxation and stress (“I feel happy”, “I feel sad”, “I feel relaxed” and “I feel stressed”) that should be answered on a 7-point scale ranging from ‘not at all’ to ‘very much’.
Next, participant in the true MBT condition will be asked to recall a recent positive event (“Think about the best and most enjoyable event since the previous set of questions. Try to imagine the event as if are experiencing it right now, as vividly as possible”). On a 7-point scale, they have to evaluate this positive event (‘very unpleasant’ – ‘very pleasant’), indicate how much they have thought about it (‘not at all’ – ‘very much’). Moreover, they have to indicate how long ago the event happened (past 30 min, 30–60 min ago, more than an hour ago) and to briefly describe the event with a minimum of 5 words using the keyboard of their smartphone (Fig. 2). We are primarily interested in the evaluation of the recalled positive event, the description is included for training specificity purposes and to ensure that participants are thinking of an actual positive event. Because we want to avoid participants actively remembering events to answer the memory question during the next prompt (true condition only), the recall of a positive event will be asked at five out of eight prompts only. In the sham MBT, participants will be asked to evaluate and describe their current location (“Think about where you right now. Look around you.”) using similar questions as in the true MBT condition at the given prompt with maximally 5 words. Again, these questions are only addressed at five out of eight prompts.
Fig. 2
Example images of the content displayed on a smartphone during ESM (A) and the designated training MBT (B), CCT (C), PVT (D), and ABT – faces (E1; face 1 = AF01 AFS and face 2 = AF26HAS) and dot-probe (E2)
To measure training-specific change in memory, memory will be assessed at two different prompts at the beginning of the first training day and at the end of the last day, by asking participants to think of a recent autobiographical event (“Think about the most important event since the previous set of questions.”) evaluate it (i.e., Recall/Evaluation Task) and to provide a brief 5-word description of this event. The last prompt of the day will include questions about the past day (“I have had fun today.”, “I am satisfied with what I have achieved today.” and “How much did you move today?”), which should be answered on a 7-point scale ranging from ‘not at all’ to ‘very much’.
Cognitive Control Training (CCT) versus active-sham CCTFor the true CCT, the PASAT will be used to exercise the maintenance of cognitive control/working memory in the face of mild frustration/negative affect and differs from episodic affective memory biases [85]. During a session, a series of single digits 1–9 is presented auditorily. Participants are instructed to continuously add each presented digit with the one that preceded it (i.e., the sum of the two last digits), and to click on the corresponding outcome (ranging from 1–18), which are presented in a diamond-shaped array (Fig. 2). The initial inter-stimulus interval (ISI) is 3000 ms, however, the PASAT is adaptive and the ISI decreases/increases by 100 ms after four accurate/inaccurate consecutive responses. As a result, the task is slightly frustrating, which is necessary to train cognitive control with increasing emotional load, while the task is adjusted to a person’s level of cognitive functioning. As such, the PASAT provides the possibility for both assessment and training of capacities [85, 86]. At each new training session, the PASAT resumes with the median ISI of the previous training.
As an active-sham CCT condition, the Peripheral Visual Training (PVT [87]) will be used to exclude potential effects of performing a computerized training. The PVT has similar characteristics to the CCT (e.g., adaptive). Participants view a circular array of colored discs (green, purple, yellow, orange or red) including an internal shape (square, circle, diamond, star, triangle, respectively) to accommodate color-blind participants, but have to keep their eyes focused on a central fixation point. Using peripheral vision (not eyes), participants have to move one disc at a time in a counter-clockwise direction in response to repeated auditory cues that signal ‘go’. When an auditory ‘stop’ cue is presented participants have to indicate the color/internal shape of this ‘stop’ cue using a button press on the smartphone. In line with the adaptive property of the PASAT, the PVT starts with a circular array of 15 discs after which one disc is added/removed after four accurate/inaccurate consecutive responses. At each new training the PVT resumes with the median number of discs of the previous session. Participants will be asked to complete either a PASAT or PVT training session of 20 min once a day for a period of 21 days.
Attentional Bias modification Training (ABT) versus sham ABTIn the ABT, two pictures (3 cm × 3 cm) of emotional faces (i.e., positive, neutral or negative) are concurrently presented on the most left and most right side of the screen (landscape orientation of smartphone with a screen width of approximately 14 cm (horizontal) × 7 cm (vertical), or scaled accordingly [67, 88, 89]. In each trial, one face is replaced by a visual probe (1 or 2 dots), to which participant are instructed to respond as soon and accurate as possible by pressing the corresponding button (1 or 2 dots) on lower left and right corner of the screen (Fig. 2). In the true (positively skewed) ABT, probes will replace 87.5% of the most positive faces of a pair, which is positive-neutral, positive–negative, or neutral-negative. Thus, participants implicitly learn to deploy attention toward positive stimuli. In the sham ABT condition, an identical procedure will be followed, except that the probe will equally often replace positive and neutral/negative faces. In line with previous work [67], participants in both conditions will be asked to complete two training sessions a day (20 min per session), for a period of 21 days. Faces for the ABT were taken from the Karolinska Directed Emotional Faces (KDEF) dataset [90].
Outcome measuresTable 1 presents an overview of the measurements across all time-points in the SMARD study.
Table 1 Overview of the measurements across all time-points in the SMARD studyPrimary outcome measuresParticipants complete one of six training conditions (MBT, CCT, and ABT vs. sham MBT, active-sham PVT and sham ABT), and all four pre- and post-training assessment measures (memory, attention, cognitive control, peripheral vision). Therefore, main outcome measures are change in memory, change in attention, change in cognitive control and change in peripheral vision. SCID-positive recurrence of depression is an additional main outcome measure during follow-up.
MemoryThe Recall/Evaluation task [73] is used to assess change in memory from pre- to post-training. In this task three prompts are given where participants are asked to think of a recent autobiographical event, describe this event, and to evaluate it briefly on a Likert scale ranging from very unpleasant (score − 3) to very pleasant (score + 3). The participant’s evaluation of each autobiographical event at pre- and post-training is used to assess training related changes in memory.
Cognitive controlFor each participant, the ISI of each PASAT trial at pre-training and each trial at post-training will be used to assess training related changes in cognitive control. In this respect, a decrease in ISI indicates improvement of cognitive control, whereas an increase indicates a deterioration of cognitive control.
Peripheral visionThe PVT, which is unrelated to cognitive control/working memory, will be used as an active control assessment [91]. Training related changes in peripheral vision from pre- to post-training will be assessed using the number of colored discs in each trial.
AttentionChange in attention from pre- to post-training is assessed using the visual dot-probe task [67] where the visual probe replaces the most positive face (congruent) in 50% of the trials and the most negative face (incongruent) in 50% of the trials. The reaction time to each probe at pre-training and at post-training is used to assess changes in attention.
Recurrence of depression and depression severityDuring the follow-up period, positive recurrences of depression will be assessed by telephone interviews every three months where the SCID-I [83] will be administered regarding the period since the last (SCID-I) assessment. Additionally, the 17-item Hamilton Depression Rating Scale (HDRS [84]) will be administered to assess severity of recurrence or residual symptoms during follow-up. The HDRS is an observer rated MDD symptom scale with 17 items, assessing depressive symptoms over the past seven days, administered as a semi-structured interview [92]. Items are scored on either a 3- (0 = absent; 1 = doubtful or mild; 2 = clearly present) or 5-point (0 = absent; 1 = doubtful or mild; 2 = mild to moderate; 3 = moderate to severe; 4 = very severe) scale, the sum score varies between 0–52.
Secondary outcome measuresA more detailed description of all questionnaires and neuropsychological tests is given in the Supplementary Material.
RuminationChange in rumination will be assessed with the Dutch version of the Ruminative Response Scale (RRS [93, 94]). The 26-item RSS assesses the tendency to engage in ruminative thinking that is focused on the self, symptoms or consequences of depressive mood. It consists of two subscales: reflective pondering and maladaptive brooding.
Neural networksA range of MRI scans will be obtained to assess training-related changes in neural networks. All scans will be made on a 3 T MRI-scanner with a 32 channel head-coil: (1) a structural scan (7 min) – a high resolution 3D T1-scan for detailed anatomic information; (2) resting-state scan (10 min); (3) Diffusion Tensor Imaging (DTI; 7 min) measures whole brain fractional anisotropy (FA) which can quantify white matter abnormalities by voxel-based analyses [95], (4) emotional reactivity will be assessed with the Hariri paradigm [96] consisting of 12 blocks (3 trials each) in which participant have to indicate which of two facial expressions (angry or fearful) presented on the bottom of the screen match the target expression of the face at the top of the screen. In 5 control blocks participants have to indicate which of two shapes (horizontal or vertical oval) presented at the bottom of the screen match the target shape at the top of the screen; (5) cognitive emotion regulation will be measured using an adapted version of the emotion regulation (ER) task used before [97, 98] during which participants view pictures of different emotion categories (negative or neutral) and are instructed to either passively view the image or actively regulate the elicited emotion by reappraising the pictures in a more positive perspective. After each picture presentation, participants have to rate their feelings and arousal level using a 5-point Self-Assessment Mannekin (SAM) scale; (6) inhibitory control will be assessed with the classic (non-emotional) Stroop Task [99, 100], in which each trial starts with a target stimulus – a color name, written in either matching (congruent) or non-matching (incongruent) ink – to which participant have to respond as quickly and accurate as possible by indicating the ink color of the word with a button press.
Training drop-out/non-complianceDrop-out (impossibility to obtain a post-training measurement and loss to follow-up) and non-compliance (number of performed training sessions relative to the total number of training sessions) rates on the MBT, CCT, ABT and respective (active-) sham conditions will be assessed.
BEHAPPBEHAPP is a smartphone application enabling longitudinal, 24/7 measures of an individual’s behavior (https://behapp.org/). The hallmark feature of BEHAPP is that it passively monitors behavior ‘in the background’; as such it can be considered a Mobile Passive Monitoring application. Passive monitoring implies that after initial informed consent and installation of the app on the smartphone, no further active input from the participant is required. A diversity of social communication and exploratory behavioral endpoint features are extracted from continuously collected smartphone sensor information such as GPS, text-messages, phone, social media (e.g., Facebook, Twitter, WhatsApp), WiFi, access (social density) signals. This data is collected at low battery-consumption. Every time the smartphone connects to WiFi, data is transferred in encrypted form to highly secured servers and wiped from the smartphone. Thus, BEHAPP enables objective behavioral observations of subjects in their natural environment. Importantly, BEHAPP never records or collects content of any spoken or written messages. Also, any identifying information related to communication partners, that is any person the participants interact with, is irretrievably obfuscated before being sent to the secured data servers. BEHAPP has been implemented in a variety of European Union (EU) projects and multi centre studies (e.g. [101, 102]) and is compliant to the General Data Protection Regulation (GDPR [82]).
Experience sampling method (ESM)Prior to the baseline assessment we will obtain 6 days with 10 semi-random measurements/day, applied via the smartphone of participants (see [103]). ESM is a structured diary method developed to study participants in their daily surroundings. We will obtain ESM-ratings regarding positive and negative affect – which are hypothesized to be separate but correlated latent factors [104] – and possible influencing factors (e.g., social activities).
ProcedureEligibility assessment, pre-training measures, randomization and post-training measureAfter expressing their interest in the SMARD study, potential participants will be contacted by telephone within a week to receive more information about the study. Those interested in further participation will receive written information about the SMARD study and an informed consent form. According to Dutch law, only after informed consent is obtained, a second appointment by telephone is made to assess eligibility (T0), including possible MRI eligibility, based on the inclusion and exclusion criteria, using the depression, psychosis, mania, anxiety, and addiction modules of theSCID-I [83]. In addition, residual depressive complaints (HDRS), the number and duration of past recurrent major depressive episodes, the type and duration of pharmacological and psychological treatment (if applicable) during past episodes, and current pharmacological and psychological treatment (if applicable) will be asked. Participants eligible for participation are invited for the baseline assessment. If participants do not want to participate in MRI-scanning or fail to meet criteria for the MRI scan, they will only be excluded for the MRI session.
At the start of the study (T1) participants receive baseline questionnaires (see Supplementary Material) by email, after which the SMARD software application (SMARD app) for the ESM assessment is installed and initialized. When the ESM assessment is obtained, participants receive instructions (written, by phone, and instruction videos) to complete four cognitive tasks (Recall/Evaluation task, PASAT, PVT, and the visual dot-probe task) on their smartphones using the SMARD app. This provides a baseline measurement of cognitive performance prior to training. For eligible participants, the first MRI-scan will be done thereafter.
After the baseline assessments, participants are randomly assigned to either MBT, MBT-sham, PASAT, active-sham PVT, ABT or ABT-sham conditions. The HDRS is re-assessed if the period between randomization and start of the cognitive training or control condition exceeds a period of three weeks. Participants will be instructed (also via written information) to complete the cognitive training either five times (MBT/MBT-sham), once (PASAT/active-sham PVT) or twice (ABT/ABT-sham) a day, for 21 consecutive days and to abstain from any psychotropic medication for ≥ 2 h before the cognitive training is started. The timing of the training during the day will be scheduled according to the individual preference of the participant. Participants will be informed that the SMARD app records (the number of) training sessions. Two to three days after the start of training, a researcher will inquire via telephone whether the SMARD app works and whether instructions are clear.
At the end of the training period (T2), participants will perform similar post-measurements as before training. They are instructed to complete the questionnaires and all four cognitive tasks (Recall/Evaluation task, PASAT, PVT, and the visual dot-probe task) delivered by the SMARD app, to acquire a post-training measurement of cognitive performance. We record potential changes in pharmacological and/psychological treatment since the start of the study. Participants who underwent pre-training MRI-scanning will again be invited for a post-training MRI scan. If participants do not complete the planned ESM assessment, cognitive tasks, or questionnaires, they receive a reminder email and/or phone call from the clinical assessor who asks them to complete the given assessment.
Follow-up assessmentsFour weeks after completing the three-week cognitive training (first follow-up assessment; T3) the HDRS is administered by phone and four smartphone-based (SMARD app) cognitive tasks are repeated in line with previous research [67]. Again, we record changes in pharmacological or psychological treatment (since T2; post-training assessment). Hereafter, a one-year follow-up period starts with 3-monthly assessments (T4-T6, T9 [endpoint]) by phone. Before each follow-up assessment, participants receive questionnaires (see Supplementary Material) by email. During each assessment we identify recurrent depressive episodes by administering the SCID-I [83] record changes in pharmacological and/or psychological treatment, and measure severity of (residual) depressive symptoms (HDRS). When a recurrence is expected/identified, participants will be advised to seek professional help. Any adverse events that occur after enrollment in the study and before the end of the follow-up period, will be recorded. An adverse event that meets the criteria for a serious adverse event (SAE) will be reported to the ethical medical committee.
Data handlingAll study-related information is electronically stored on secured servers (Google Cloud or within the Radboud university medical centre) with access by involved researchers only. Questionnaire data, demographic data, data on previous MDD episodes and treatment is collected, stored and managed via Castor EDC. For Castor EDC, full audit trail is available to log change(s) to the data as well as which user (researcher) made the change. To ensure anonymity and confidentiality, all data is anonymized with a unique participant ID code. The key file linking this participant ID to personal information is stored in a separate, password-protected file at the Radboud university medical centre. Only researchers, an independent monitor from the Radboud university medical centre and the Inspection for Healthcare and Youth have access to these key files. Smartphone data of cognitive trainings, ESM and BEHAPP will be uploaded anonymously to the Google Cloud Platform, which employs a security model built on 15 years of experience in protecting customer data. This platform is compliant with HIPAA, ISO 27001 and the EU Data Protection Directive. No directly identifiable participant information is stored. Participants are represented by unique IDs, which can only be associated with identifiable information via the key to these IDs, stored at Radboud university medical centre. BEHAPP monitoring data is encrypted before being locally stored on the smartphone and after each successful upload to the BEHAPP servers, all of the local monitoring data is wiped from the smartphone. Likewise, data of cognitive trainings and ESM are uploaded after each task and then cleared from the smartphone. These measures seek to maximally reduce the risk of revealing privacy-sensitive information to third parties in case of loss or theft of the smartphone. Information gathered about identities of third persons, for example participants’ contacts, are obfuscated on the phone before being uploaded to BEHAPP servers. Obfuscation is performed using so called one-way-hashing/encryption techniques. This allows the researchers to determine whether the same instance (person or device) has been recorded more than once, while preventing them from directly identifying the recorded instance.
Data will be stored for 15 years after participant inclusion has ended. Only researchers who are part of the research team are able to access the data. The study has low to negligibly risks therefore the monitoring plan will be performed in line with the Radboud university medical centre regulations and the procedures as described in the brochure “Kwaliteitsborging mensgebonden onderzoek 2.0” by the Dutch Federation of Universities (NFU). Results of the SMARD study will be published in (inter-)national, peer-reviewed scientific journals, and presented at (inter-)national conferences. Moreover, participants will receive a summary of the study results.
Statistical analysesFollowing the Consolidated Standards of Reporting Trials (CONSORT [105]) all primary and secondary outcome analyses will first be conducted in accordance with the intention-to-treat (ITT) principle. Second, we will perform an analysis to explore dose–response relationships of trainings (with percentage of completed training sessions as covariates) followed by a per-protocol analysis where we will analyze effects only in participants who completed ≥ 80% of trainings. Missing values (except for incomplete training sessions or loss to follow-up) will be imputed (e.g., by using multiple imputation (MI) or expectation maximization (EM)). In addition, sensitivity analyses will be carried out to gauge the robustness of findings as a result of including/excluding participants with missing data in the analysis. In case cognitive training groups differ regarding potential confounders, despite randomization, these variables will be added as covariates in the analyses described below.
Primary outcome analysesThe effects of cognitive training (MBT vs. sham MBT, CCT vs. active-sham CCT, ABT vs. sham ABT) on the primary outcome measures will be analyzed using linear mixed-effects models (LMEM). LMEM are ‘mixed-effects’ models as they consider both fixed and random effects. Fixed effects are parameters that do not vary across units of interest (e.g., participants or stimuli). Random effects, however, are parameters that do vary across units of interest. Random effects include random intercepts (i.e., variation of intercepts) and random slopes (i.e., variation in the relation between the independent variable(s) and dependent variables), Disregarding these random effects may lead to inflated Type-I error rates [106], which is why LMEM is preferred over traditional analysis of variance (ANOVA) techniques that only consider fixed effects [107, 108]. Moreover, LMEM analyze data on the trial level instead of aggregating data (e.g., mean/median reaction time of all trials of a visual dot-probe task).
Here, four separate LMEM will be conducted (Table 2) on trial level dataFootnote 3 using R statistical computing language [109]. Each model will include one of the outcome measures as the dependent variable (model 1: Memory (Recall/Evaluation Task); model 2: Cognitive control (PASAT); model 3: Peripheral vision (PVT); model 4: Attention (visual dot-probe task)). All models will have the independent variables Time (pre-training, post-training) and Training condition (MBT, sham MBT, CCT, active-sham CCT, ABT, sham ABT) as fixed effects. In addition, a random intercept for Participant and a random slope for Time will be included as random effects.
Table 2 R Syntax of planned analysesFurthermore, for the dependent variable in the PVT (model 3) color/shapeFootnote 4 will be included as an additional random intercept with a random slope of Time. Likewise, the dependent variable Attention (model 4) will include the independent variables Stimulus valance (happy, neutral, angry, sad) and Congruency (congruent, incongruent) as fixed effects. This model will also include a random intercept for Participant and a random intercept for Actor ID, with random slopes for Time, Stimulus valance and Congruency, as well as the interaction between Time, Stimulus valance and Congruency varying over Participant and over Actor ID.Footnote 5 For all of the models outlined above, the interaction effect(s) and all lower order effects will be analyzed.
Investigation of the association between passive behavioral data (BEHAPP) and recurrencesIn order to predict positive recurrences of depression during follow-up, the multidimensional data obtained by BEHAPP will be associated with SCID-I positive recurrences of depression as determined during follow-up. To this end, multivariate pattern recognition machine learning will be used to develop an algorithm that can distinguish behavioral aspects associated with a depressed versus non-depressed state. This algorithm will be developed to identify an individual’s behavioral changes characterizing an evolution from a non-depressed state towards recurrence. Algorithms to detect changes in activity [110] and/or indications for directions of signals [111] exist. We will especially investigate whether early changes in behavior can be detected in the weeks before the recurrence becomes evident. Finally, the algorithm will be improved such to obtain highest sensitivity (at reasonable specificity). With ongoing/additional data collection of the SMARD study, we aim to replicate and improve the algorithm. For example, with knowledge of medication use of participants and an increasing dataset, we can investigate whether medication use modifies our predictions by performing stratified analyses to obtain predictive algorithms, and to compare these with the overall prediction. Finally, we will investigate possibilities to develop improvement of the algorithm into a self-learning system.
Secondary outcome analysesEffects on the secondary outcomes change in rumination (RRS) and depressive severity (HDRS) will also be analyzed by means of LMEM. Two models (see Table 2) will be conducted including the outcome measure as dependent variable (model 5: Rumination (RRS); model 6: Depressive symptoms (HDRS)). Both models include the independent variables Time (pre-training, post-training) and Training condition (MBT, sham MBT, CCT, active-sham CCT, ABT, sham ABT) as fixed effects, and a random intercept for Participant and a random slope for Time as random effects. For these two models, the interaction effect and all lower order effects will be analyzed.
Power and sample sizeThe power analyses described here are based on repeated-measures ANOVA as for LMEM no power calculations have been specified, except for data simulations. For our primary outcome
Comments (0)