
Remember me


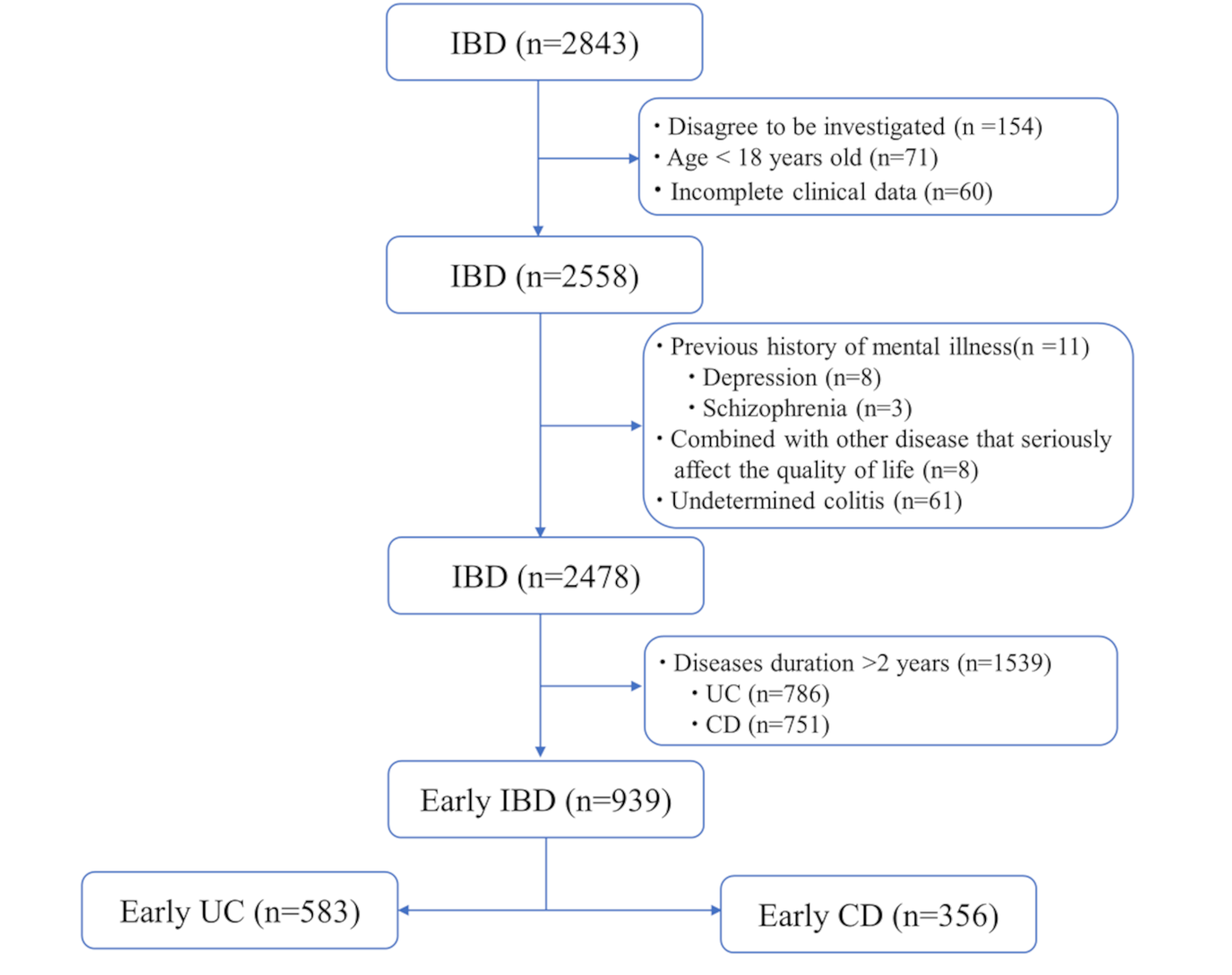
A total of 939 early patients with IBD were included in the study, comprising 583 patients diagnosed with UC and 356 patients diagnosed with CD. The average age of these patients was 34.0 years (27.0–43.0), and the average weight was 60.0 kg (54.0–70.0). Male patients (59.6%) outnumbered female patients (40.4%). Table 1 presents the sociodemographic characteristics, disease features, and treatment modalities of early UC and CD patients. Significant differences were observed between early UC and CD patients in terms of age, weight, gender distribution, proportion of initial visits, disease activity, intestinal symptoms, treatment modalities, and income level (p < 0.05). Consequently, subsequent analyses should separately address early UC and CD patients.
Table 1 Clinical characteristics of early patients with IBDPsychological symptoms and quality of life in early patients with IBDIn early patients with IBD, early UC patients exhibited slightly higher GAD-7 and PHQ-9 scores compared to CD patients. Conversely, early UC patients had marginally lower scores on the IBD-Q and PSQI than CD patients. The GAD-7, PHQ-9, PSQI, and IBD-Q scores of early patients with IBD are shown in Fig. 2. After categorizing early patients with IBD based on the cutoff values of questionnaire score, 20.3%, 21.7%, 57.3%, and 41.9% of early patients with IBD exhibited symptoms of anxiety, depression, sleep disturbances, and poor QoL, respectively. Additionally, 15.2% of patients experienced comorbid anxiety and depression (Table 2).
Fig. 2
PHQ-9 score (A), GAD-7 score (B), PSQI score (C), and IBD-Q score (D) of early patients with IBD, IBD-Q score including 4 dimensions of bowel symptoms (E), systemic symptoms (F), emotional ability (G), and social ability (H)
PHQ-9, Patient health questionnaire-9; GAD-7,Generalized anxiety disorder-7; PSQI, Pittsburgh sleep quality index; IBD‐Q, inflammatory bowel disease quality‐of‐life questionnaire; CD, Crohn’s disease; IBD, inflammatory bowel disease; UC, ulcerative colitis
Table 2 Psychological symptoms and quality of life in early patients with IBD, UC and CDAmong early UC patients, 131 (22.5%) had anxiety, 136 (23.3%) had depression, 330 (56.6%) had sleep disturbances, and 271 (46.5%) had poor QoL. In comparison, early CD patients had 60 (16.9%) with anxiety, 68 (19.1%) with depression, 208 (58.4%) with sleep disturbances, and 122 (34.3%) with poor QoL. The proportion of UC patients with anxiety and poor QoL was higher than that of CD patients (P < 0.05), while no significant differences observed between the two groups concerning depression and sleep quality.
Factors influencing psychological symptoms in early patients with IBDTo further elucidate the factors influencing psychological symptoms in early patients with IBD, we conducted univariate logistic regression analyses for early IBD (Supplementary Table 2), including UC and CD. The results showed that for early UC patients, factors such as weight loss, first visit, poor QoL, hematochezia, and residing in the eastern region could affect patients’ anxiety levels. In terms of depression, factors such as being female, first visit, low income level, residing in the eastern region, and poor QoL were significant. while factors like gender, first visit, steroid use, disease activity, low incomes level, and residing in the eastern region could influence sleep disturbances (Table 3). As for early CD patients, factors such as gender, high disease activity, and poor QoL could affect anxiety levels. Furthermore, increasing age, disease activity, and poor QoL were associated with depression and sleep disturbances (Table 4).
Table 3 Univariate logistic regression of influencing factors of psychological symptoms in early UC patientsTable 4 Univariate logistic regression of influencing factors of psychological symptoms in early CD patientsConsequently, we performed multivariate regression analysis to identify independent factors influencing psychological symptoms in early patients with IBD (Fig. 3A, B, and C). For early UC patients, the timing of the first visit, hematochezia, and poor QoL emerged as independent factors contributing to anxiety symptoms. Depression symptoms were independently influenced by the timing of the first visit, female gender, residence in the eastern region, and poor QoL. Sleep disturbances were primarily affected by disease activity and residential region (Fig. 3D, E, and F). For early CD patients, high disease activity and poor QoL were independent factors influencing anxiety symptoms. For depression, increasing age and poor QoL were independent factors, while sleep quality was predominantly affected by poor QoL (Fig. 3G, H, and I).
Fig. 3
Forest plot of multivariable analysis results of anxiety (A, D, G), depression (B, E, H) and sleep disturbance (G, H, I) symptoms in early IBD, UC, and CD patients
The correlation between GAD-7, PHQ-9, and PSQI and IBD-Q in early patients with IBDWhen analyzing the influencing factors of psychological symptoms in early patients with IBD, we observed that poor QoL has a certain impact on all psychological symptoms.
To further investigate the relationship between psychological symptoms and QoL in early patients with IBD, we conducted a correlation analysis between the scores of the IBD Quality of Life (IBD-Q) and its four components and the scores of the psychological symptom questionnaires in early patients with IBD. Spearman correlation analysis revealed that for early patients with IBD, their IBD-Q score was significantly correlated to their PHQ-9 score (r=-0.3, P < 0.001), which was mainly mediated by the IBD-Q systemic symptoms (r=-0.32, P < 0.001) and the emotional ability score (r=-0.33, P < 0.001). Although the GAD-7 score did not show a significant correlation with the total IBD-Q score, it was closely related to the emotional ability score of the IBD-Q (r=-0.32, P < 0.001) (Fig. 4A). No significant correlation was found between the PSQI score and the IBD-Q score (P > 0.05). In the analysis of IBD subtypes, no significant correlation was found between psychological symptom questionnaire scores and IBD-Q scores in early UC patients (P > 0.05) (Fig. 4B). However, in early CD patients, the results showed the opposite pattern (Fig. 4C). The IBD-Q score and GAD-7, PHQ-9, and PSQI scores of early CD patients were significantly correlated. Among them, the emotional ability score was significantly correlated with GAD-7 (r=-0.46, P < 0.001) and PHQ-9 score (r=-0.44, P < 0.001), and the systemic symptoms score was significantly correlated with PHQ-9 score (r=-0.42, P < 0.001) and PSQI score (r=-0.4, P < 0.001). These results indicate that when further exploring the impact of QoL on psychological symptoms based on questionnaire scores, the IBD-Q scores for emotional ability and systemic symptoms only affect the depression and anxiety scores of early patients with IBD and the psychological symptom scores of early CD patients, and are not related to those of early UC patients. Improving the QoL for early patients with IBD will reduce their risk of psychological symptoms, especially for early CD patients. This further explains the differences between UC and CD as different subtypes of diseases in terms of pathophysiological mechanisms and influencing factors of psychological symptoms.
Fig. 4
The correlation between the psychological symptoms scores and IBD-Q and it’s four dimensions in early IBD (A), UC (B), and CD (C) patients. Note: psychological symptoms scores refer to GAD-7, PHQ-9 and PSQI score;
The factors influencing poor quality of life in early patients with IBDGiven the impact of psychological symptoms on the QoL of early patients with IBD, we included these symptoms in our analysis and used logistic regression to explore all possible factors influencing their QoL. The univariate analysis showed that age, first visit, diagnosis type, anxiety, depression, sleep disturbances, disease activity, diarrhea, abdominal pain, hematochezia, income level and all psychological symptoms were factors affecting the QoL of early patients with IBD (Supplementary Table 3). Therefore, we further conducted a multivariate analysis, and the results showed that depression was the only psychological symptom identified as an independent factor affecting QoL in early IBD patients. Other factors included first visit, disease activity, abdominal pain, hematochezia and income level. In addition, the results of subtype analysis showed that the extraintestinal manifestations (EIM) and sleep disturbances significantly impacted QoL of early UC and CD, respectively (Table 5).
Table 5 Multivariate logistic regression of influencing factors of poor quality of life in early patients with IBDConstruction and validation of a nomogram model for the poor QoL of early patients with IBDBased on the factors influencing the QoL of early patients with IBD, we constructed a nomogram model for predicting poor QoL in training cohorts of early patients with IBD, UC and CD, separately. The results of the difference analysis showed no statistical differences between the training and validation groups in various indicators, making them suitable for further analysis (Supplementary Table 4).
The nomogram model constructed based on the factors influencing the QoL of early patients with IBD revealed that disease activity and economic status were the most significant factors affecting the QoL of early patients with IBD, with the highest proportions in the model. Results from 1000 repetitions of Bootstrap sampling showed a good fit between the actual curve and the ideal curve of the model, with a C-index of 0.780. The ROC curve analysis yielded an AUC of 0.781 (95% CI: 0.748–0.814), demonstrating robust discriminative power. The DCA curve results showed excellent clinical utility of the model within the range of 16–85%(Fig. 5). Similarly, the predictive nomogram models for the QoL of early UC and CD patients also demonstrated good discriminative ability and clinical utility. In the training group, both nomogram models showed good fits with the actual and ideal curves, with C-index values of 0.780 and 0.824, and AUC values of 0.781 (95% CI: 0.740–0.822) and 0.825 (95% CI: 0.770–0.879), respectively. The DCA curve results indicated good clinical utility within a certain range. The nomogram model based on risk factors showed good clinical practical value (Figs. 6 and 7).
Fig. 5
Nomogram (A), calibration curve (B), receiver operating characteristic curves (C) and decision curve analysis (D) used to predict poor QoL in Early patients with IBD
Fig. 6
Nomogram (A), calibration curve (B), receiver operating characteristic curves (C) and decision curve analysis (D) used to predict poor QoL in Early UC patients
Fig. 7
Nomogram (A), calibration curve (B), receiver operating characteristic curves (C) and decision curve analysis (D) used to predict poor QoL in Early CD patients
Furthermore, we further validated our model performance using the validation dataset. In the validation cohort, our model showed good performance in terms of AUC values and other evaluation metrics, demonstrating the stability of our model for clinical application (Figures S1). Additionally, we compared our model with an existing QoL prediction model for patients with IBD, which considers factors such as first visit, psychological symptoms, gastrointestinal symptoms, and disease activity [18]. The comparison focused on two key metrics. The NRI and IDI values indicated that our nomogram model provided superior discriminatory performance compared to the existing model, effectively reclassifying patients into more accurate risk categories, and supported the improved accuracy of our model in predicting poor QoL. (Table 6), Specifically, the NRI and IDI of our model were 0.324 (95% CI: 0.196–0.451, P < 0.001) and 0.026 (95% CI:0.014–0.038, P < 0.001) for early patients with IBD. Similarly, the NRI and IDI indices for early UC patients’ QoL prediction model were 0.366 (95% CI:0.207–0.525, P < 0.001) and 0.032 (95% CI:0.017–0.047, P < 0.001), respectively. For early CD patients’ QoL prediction model were 0.437 (95% CI:0.240–0.635, P < 0.001) and 0.033 (95% CI:0.010–0.056, P = 0.006), indicating that our model can more accurately identify early patients with IBD at risk for poor QoL, and our model includes fewer indicators, making it more easily applicable and promotable in clinical settings.
Table 6 The NRI and IDI of nomogram model of poor QoL in early IBD, UC and CD patients
Comments (0)