
Remember me

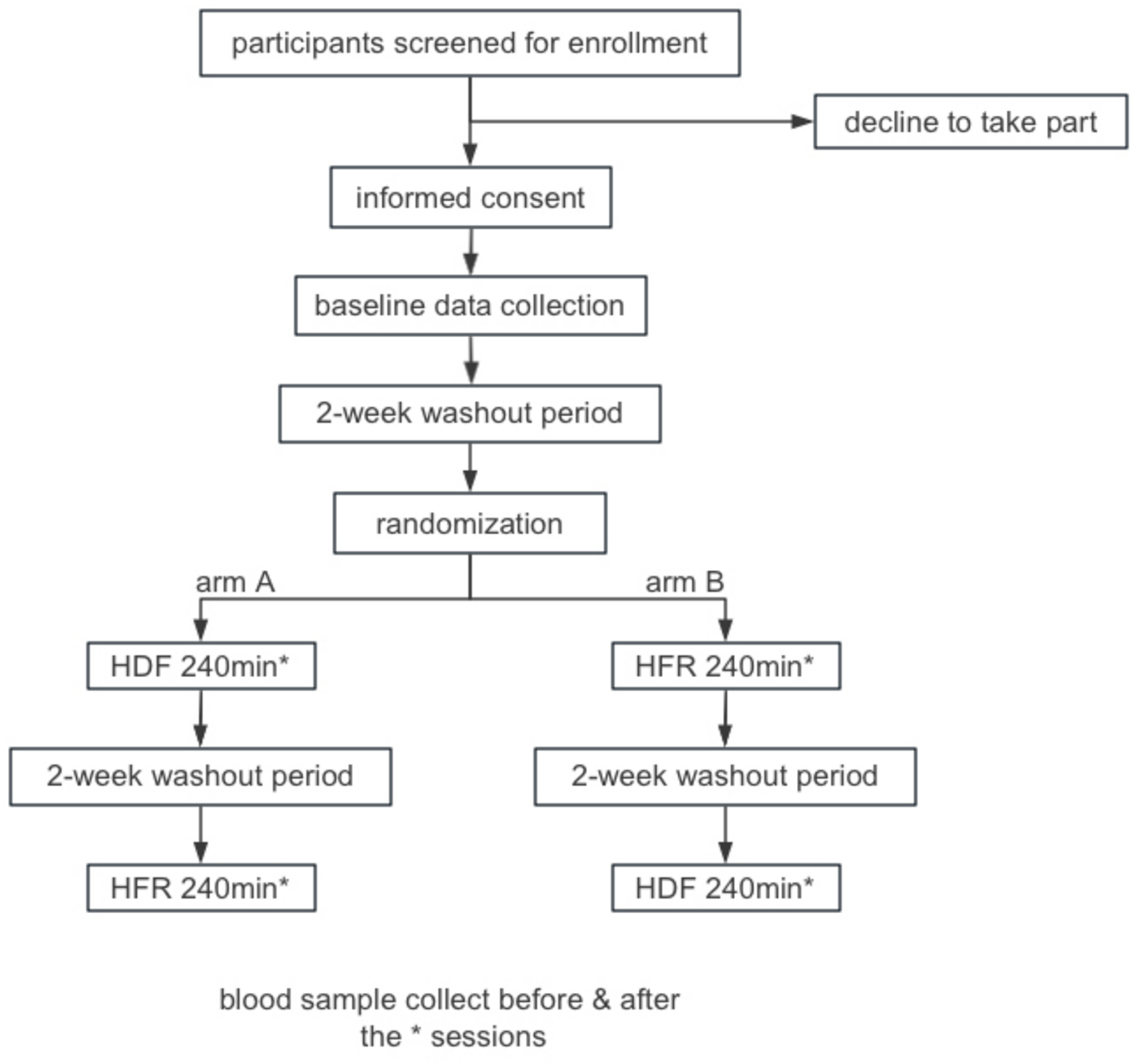



This study is a single-centered, open-label randomized controlled trial. (Figures 1 and 2) The study proposal was approved by the institutional review committee of the Naval Medical Center of PLA (registration number: 2024123104). The study will be conducted in accordance with the local legislation and institutional requirements. The research has been registered in chictr.org.cn (ChiCTR2500096698).
Fig. 1 Fig. 2
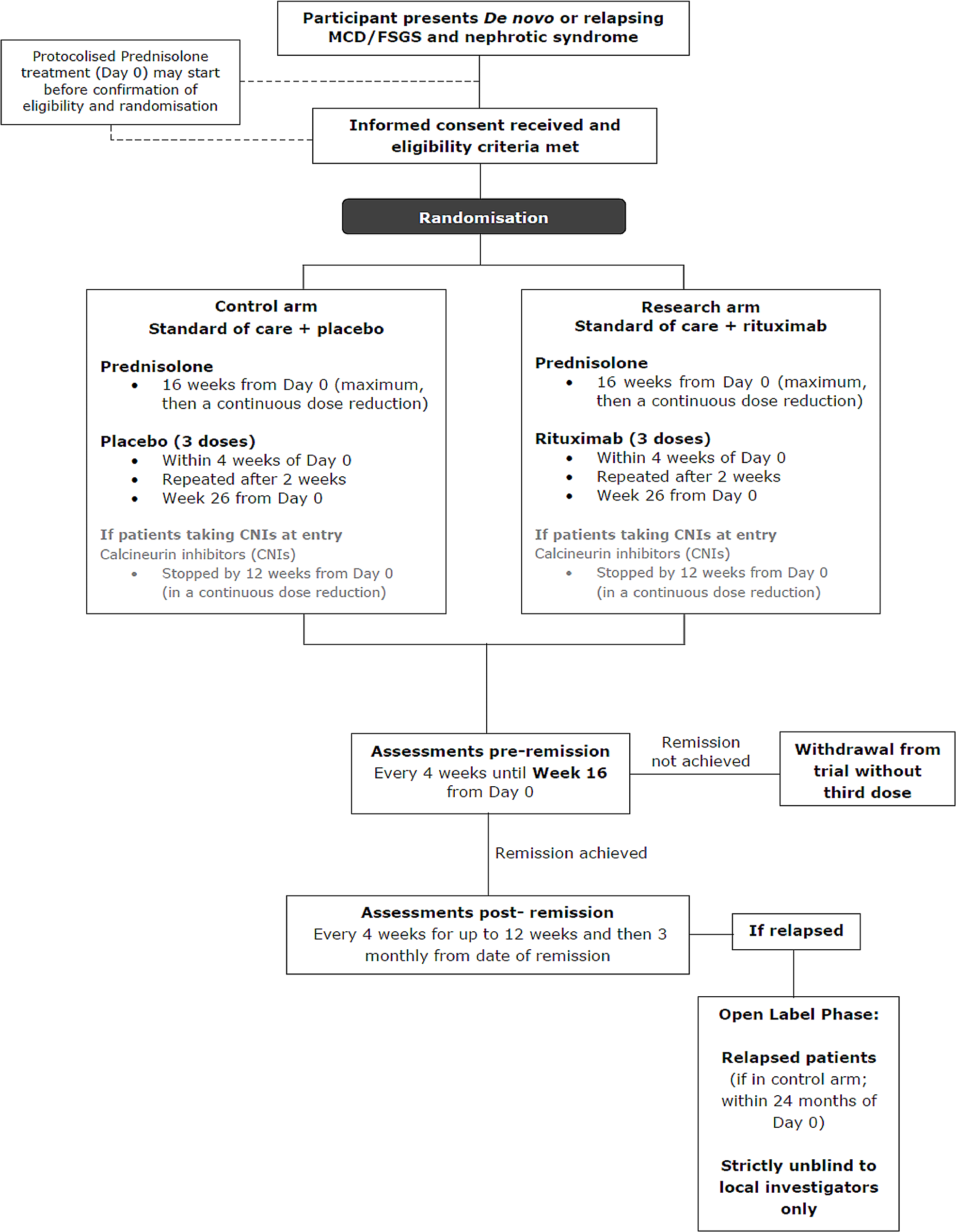
Fig. 2
Schedule of enrolment, interventions, and assessments
Study populationSample sizeSample size calculation was performed using G*Power 3.1 software. The assumed effect size of 0.45 was derived from a previous randomized controlled trial [16]. To achieve 80% statistical power (1-β) and an effect size of 0.45, with a significance level (α) of 0.05, the sample size calculation suggested a minimum of 26 participants. We opted to recruit 30 participants, ensuring at least 15 individuals per group.
Inclusion and exclusion criteriaInclusion criteria 1): patients who are 18 years or older. 2): patients on maintenance HD for three times/week in naval medical center of PLA. 3): patients who have signed an informed consent form. Exclusion criteria: 1): patients combined therapy with peritoneal dialysis and HD. 2): patients who underwent general anesthesia surgery within the past week. 3): patients on any unstable clinical conditions. 4): patients with known malignancy or severe liver disease. 5): patients who are unable to eat orally.
Baseline data collectionBefore washout, baseline data will be collected from all enrolled patients. Baseline data will include demographic characteristics and clinical background. Demographic characteristics will encompass sex, age, height, and weight, among other relevant factors. Clinical background include: primary renal failure cause, dialysis duration, complications, comorbidities such as cardiovascular disease, diabetes, and stroke. Laboratory tests at baseline are also considered: iron metabolism markers, brain natriuretic peptide (BNP), pro-BNP, albumin, C-reactive protein, blood urea nitrogen, prealbumin, total cholesterol, hemoglobin, corrected calcium, phosphorus, and parathyroid hormone.
Blinding and randomizationAfter the two-week HD washout period. The randomization procedure will be performed by Dan Ye using a random number generator computer program (Microsoft Excel for MacOS, Version 16.94). The randomization sequence will be concealed using opaque envelopes from both the study participants and the researchers responsible for enrolment and assignment until the moment of treatment allocation. This process ensures that no information about group allocation is available before assignment, preventing any bias in the allocation process. The included patients will be assigned to arm A and arm B in 1:1 ratio. Maintaining blinding of the researchers responsible for implementing the interventions is not feasible. However, to ensure the integrity of the data, the researchers tasked with data analysis will remain blinded until the completion of all data analysis procedures. After randomization, patients in arm A will first receive HDF treatment for 240 min, followed by a 2-week washout period with conventional HD, after which they will undergo HFR treatment for 240 min. Conversely, patients in arm B will first receive HFR treatment for 240 min, followed by a 2-week washout period with conventional HD, and then undergo HDF treatment for 240 min. This design aims to minimize potential bias due to the sequence of treatments. The date of HDF or HFR treatment will be defined as Day D or Day R, respectively, with the requirement that the previous HD session occurs on Day D-2 or Day R-2.
InterventionsLow molecular weight heparin is the anticoagulant of choice, with dosing adjusted per routine clinical practice to maintain circuit patency. The blood flow rate is maintained at a minimum of 200 mL/min throughout the treatment. While this is the minimum acceptable rate for the study, clinicians will be encouraged to target higher blood flow rates (e.g., 250–350 mL/min) as tolerated by the patient’s vascular access to optimize clearance, consistent with standard practice. The dialysate flow rate is consistently set at 500 mL/min. Each treatment session is standardized to a fixed duration of 240 min. Dialysis adequacy (e.g., spKt/V) will be monitored quarterly as per standard unit protocol but is not a primary outcome measure for comparing HFR and HDF in this study focused on micronutrients. The ultrafiltration volume is individualized based on the patient’s condition, though it is recommended that it not exceed 5% of the patient’s dry weight unless clinically indicated and carefully monitored.
Safety monitoring and halting criteriaPatients will be monitored throughout the dialysis sessions according to standard clinical practice, including vital signs and circuit pressures. The HDF or HFR treatment will be halted prematurely under the following circumstances: severe hypotensive episode unresponsive to standard intervention, acute allergic reaction, persistent access issues preventing target blood flow, irremediable circuit clotting, or any other acute event deemed clinically significant by the attending nephrologist and data from the incomplete session may be excluded from the primary analysis depending on timing and reason for stoppage.
HDF protocolFor the HDF treatment, the Fresenius 5008 S HD machine and the FX80 dialyzer will be utilized. Post-dilution online HDF will be performed with a target substitution fluid volume appropriate for the treatment time and blood flow rate.
HFR protocolThe HFR treatment will be administered using the Formula Dialysis Therapy machine (Bellco, Italy). Central to the HFR technology are two essential components: the dual-chamber filter, Supra17 (Bellco, Italy), and the resin adsorption column, Suprasorb (Bellco, Italy).
Outcome measuresBlood samplingBlood samples will be collected from each patient both before and after HDF and HFR treatments. Blood sampling will be performed immediately prior to starting the treatment, followed by initiation of the dialysis procedure. The method for post-treatment blood sampling will follow the protocol recommended by the KDOQI guidelines [17, 18]: at the end of the treatment, the dialysate flow rate will be reduced to zero, and the blood flow rate will be decreased to 100 mL/min for 15 s, after which the blood pump will be stopped and the sample collected. All the analyses will be conducted in Kingmed diagnostics, Inc. Guangzhou, China.
Primary outcomesTrace elements level: Iodine (inductively coupled plasma mass spectrometry).
Secondary outcomesTrace elements level: Cu, Mg, Zn, Se, Fe, Ca, Pb, Cd (inductively coupled plasma mass spectrometry).
Water-soluble vitamins level: riboflavin, niacin, pantothenic acid, pyridoxine, folate, cobalamin (high-performance liquid chromatography-tandem mass spectrometry) and biotin (high-performance liquid chromatography).
Fat-soluble vitamins level: vitamins E (ultra-high performance liquid chromatography), K, ergocalciferol, and cholecalciferol (high-performance liquid chromatography-tandem mass spectrometry).
Statistical analysesDescriptive statistics will be used to summarize baseline characteristics and outcome measures. Continuous data will be presented as mean ± standard deviation (SD) for normally distributed variables and as median (interquartile range, IQR) for non-normally distributed variables, and frequency (percentage) for categorical variables. Normality will be assessed using the Shapiro-Wilk test.
Baseline demographic and clinical characteristics between the two treatment groups (Arm A and Arm B) will be compared. For continuous variables, an independent t-test (for normally distributed data) or Mann-Whitney U test (for non-normally distributed data) will be used. For categorical variables, the Fisher’s exact test will be applied.
The primary analysis will focus on the primary endpoint: the change in serum Iodine level from pre-treatment to post-treatment. Repeated measures ANOVA will be used, with treatment (HDF vs. HFR) and treatment period (first vs. second) as within-subject factors. The model will account for subject variability as a random effect. Covariates such as age, sex, ultrafiltration volume, dialysis vintage, and baseline I levels will be included to adjust for potential confounders.
Analyses of all other micronutrients (trace elements: Cu, Mg, Zn, Se, Fe, Ca, Pb, Cd; water-soluble vitamins: Vitamin C, B1, B2, B6, B12, Folic acid; fat-soluble vitamins: Vitamin A, D, E, K) are considered secondary and exploratory. The same repeated measures ANOVA model structure will be applied to these secondary outcomes. Given the number of secondary endpoints relative to the sample size, these results will be interpreted with caution due to the increased risk of Type I error from multiple comparisons. For a limited number of pre-specified key secondary outcomes (e.g., Selenium, Folate), we may apply adjustments for multiple comparisons (such as Bonferroni or False Discovery Rate methods) and will report both adjusted and unadjusted p-values, noting the exploratory nature of these analyses. Sensitivity analyses may explore alternative approaches like ANCOVA on the change scores if model assumptions for repeated measures ANOVA are significantly violated. Statistical significance will be defined as p < 0.05, and all analyses will be conducted using SPSS Statistics for MacOS, version 30.0.0.0 (SPSS Inc., Chicago, IL, USA). Data access will be restricted to the principal investigators, designated study coordinators, and the blinded statistical analysis team. Data will be stored securely according to institutional guidelines.
Comments (0)