The overseas KT is a significant international concern [8]. The primary reason for seeking KT abroad was the lack of available donors. In our study, we observed unfavorable outcomes in the commercial KT group, in the form of higher incidence of surgical complications (SSI and lymphocele) as well recurrent UTI. Moreover, this Group had a higher rate of acute rejection episodes. This could be explained by the inappropriate induction immunotherapy protocol in the form of improper selection according to the patients’ immunological risk [5], or the inadequate dose as most of these patients were discharged from the transplant center within 3 days.
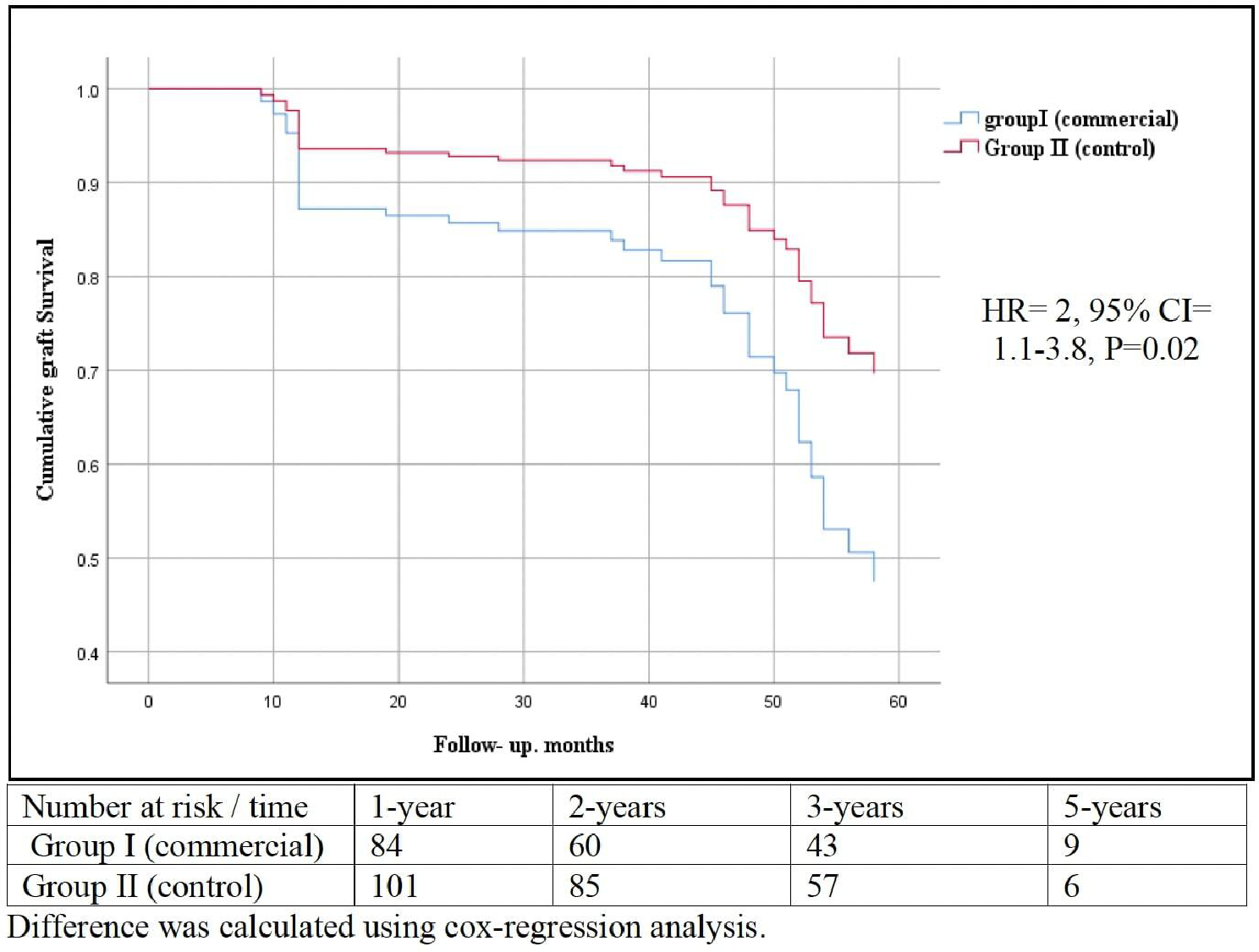
Consequently, the 1-year patient survival was significantly lower in commercial KT group compared to the control group and to the reported 1-year survival rate of 98.4% of living KT in Saudi Arabia [9].
There are conflicting reports regarding the outcomes of patients receiving commercial KT, with both unfavorable and favorable results documented [10]. Several international studies have reported favorable outcomes, including one of the most extensive analyses comparing graft and patient survival rates. In 2000, Morad et al. examined Malaysian patients (n = 515) who underwent commercial KT from either live of deceased donor and compared them to 258 local live-donor KT. He reported comparable patient and graft outcomes at 1, 3, and 5 [11]. In our study, graft survival and patient outcomes were significantly better in the local transplant group. However, overseas KT may carry additional risks and complications, but it still offers better long-term survival and quality of life than remaining on dialysis.
Recent studies show that commercial KTs often have worse outcomes. For example, sever et al. followed 115 patients who received commercial KTs (mostly from unrelated donors) in countries like India, Iran, and Iraq [12]. Alarmingly, 15 patients got unusual infections (malaria, fungal infections), and long-term results were poor: a 7-year graft survival (53% vs. 73% for living-related KTs at their center) and 7-year patient survival (74% vs. 80% for living-related KTs) [12].
While patient survival was similar to other commercial KTs, graft survival was worse [12]. Another study of 16 patients found even higher risks: 1-year survival: 80–96% (much lower than the > 95% seen in living-related KTs) and 5-year survival: Just 60% [13]. Moreover, many patients had severe infections (hepatitis B, drug-resistant bacteria, and fungal infections) [13]. Our study, however, did not see these unusual infections in commercial KT patients—possibly due to stricter screening.
Additionally, Sajjad et al. highlighted that some commercial transplant centers may have suboptimal surgical conditions, potentially increasing infection risks. In our study, we observed a significantly higher incidence of surgical site infections (P = 0.03), lymphocele (P = 0.007), and urinary tract infections (P = 0.002) in Group I. While we cannot confirm the specific conditions of the transplant centers where these patients received their organs, the increased infection rate in Group I suggests that factors such as perioperative management, sterility protocols, and post-operative care may have contributed to these outcomes. Meanwhile, donors are mainly from lower socioeconomic groups in developing countries who often need more access to follow-up care. In some instances, these donors may even carry infectious diseases such as tuberculosis, AIDS, and hepatitis [3].
De Souza et al. reported a 1-year infection rate of 42.2%, with UTI being the most common. This finding is consistent with the established view that UTI are the most prevalent infections among patients undergoing KT [14]. Similarly, in our cohort, patients who underwent overseas commercial KT had higher rates of SSI and UTI rates.
The onset of acute rejection significantly reduces long-term graft survival, especially if rejection is not completely reversed [15]. In our study, seven patients who underwent overseas KT experienced graft rejection, whereas only two patients from the local cohort experienced similar issues. Because overseas KT is often commercially motivated, patients at these centers typically experience the shortest postoperative hospital stay and are encouraged to return to their home countries upon discharge which affect the protocol of IS induction [5].
Study limitations
The primary limitations of our study include the small sample size and the fact that it was conducted at two centers. Moreover, the age difference between Group I and Group II patients is a potential confounder of some outcomes, such as infections and length of hospital stay. Furthermore, the observational and retrospective designs with the inherent selection bias, however such studies cannot be performed in a prospective manner. One of the major limitations is the lack of detailed data regarding the induction immunosuppressive (IS) therapy administered to patients in Group I. While we inferred suboptimal induction protocols from the high rejection rates, the absence of precise documentation on IS regimens limits our ability to draw definitive conclusions. Additionally, our study did not quantify the number of patients with very low calcineurin inhibitor (CNI) levels upon arrival. However, our findings suggest that inadequate immunosuppression contributed to poorer outcomes.
Another complicating factor is the multiple locations where the transplants in Group I were performed. The variability in surgical expertise, perioperative management, post-operative care, and local healthcare infrastructure likely influenced the observed outcomes, making direct comparisons between the groups more complex. The unavailability of warm and cold ischemia times for Group I is another limitation, as ischemia time significantly affects transplant outcomes.





Comments (0)