Over the past 2 decades, multiple popPK models of ceftriaxone for pediatric patients have been reported in literature [3,4,5,6,7]. Among these models, some have described ceftriaxone disposition in the critically ill pediatric population [3, 5]. However, until now, these models have not been externally validated to prove applicability. For this external validation, data acquired through the EXPAT Kids study were used to evaluate predictive performance [16]. Our results show that the ceftriaxone popPK model by Khan et al. performed best using our external population in relation to the performance metrics [3]. However, none of the models showed a clear trend toward over- or underprediction of ceftriaxone concentrations. Both models for unbound ceftriaxone concentrations, by Hartman et al. and Tang-Girdwood et al., performed inadequately [3, 5]. These findings highlight that, despite apparent similarities in patient characteristics, differences in PICU admission criteria and antibiotic quantification methodologies could significantly impact a model’s generalizability and may lead to suboptimal description of concentration-time profiles. Consequently, our results underscore the importance of externally validating the popPK model in the target population before the model is applied for MIPD, as was acknowledged in similar recently published external evaluation studies [19,20,21].
The performance evaluation did not indicate a clear preference for any specific popPK mode. This might largely be explained by the large variability within the critically ill pediatric population. Two popPK models were developed in a PICU population, the Wang et al. model was built with pediatric patients aged 1 month to 2 years with suspected or confirmed bacterial infection, while the Khan et al. model had a wider age range (2–12 years) with patients who were confirmed or suspected of having pneumonia [6, 7]. All model populations received 50 mg/kg and/or 100 mg/kg every 24 h or every 12 h, except for the Wang et al. model, where the median dose was 30 mg/kg. Our dataset consists of PICU patients receiving 100 mg/kg every 24 h, with a wide range of clinical indications, feeding the assumption that the Hartman et al. and Tang Girdwood et al. models would fit best when considering study populations.
“Correct” model selection is primarily guided by the intended purpose of the model. For example, the appliance may be aimed at guiding individualized dosing in a specific clinical setting, informing drug development decisions, or providing insights into variability in drug exposure within specific populations. These goals influence decisions on structural model development and complexity, covariate selection, and the use of specific datasets. Though less effective when all models are biased (i.e., under- or overexposure), choosing multiple models over a single model to interpret a patient’s PK might be beneficial. Model averaging and model ensembling are new statistical approaches that weight models on the basis of their ability to describe the data, the demographics of the population, and other parameters to select the most optimal model or weighted combination of models when using MIPD [22,23,24]. However, if all models over- or underpredict, model re-estimation may be an alternative method for preventing new model development, especially when published models display similar model parameters and covariate relationships [25].
Owing to differences in the study population (covariate ranges), extrapolation of covariate relationships may have resulted in decreased accuracy of model predictions. An example of this may be the age range within the included model (Wang et al. range 0.10–1.99 years) and the external evaluation dataset (EXPAT Kids study, 0.1–17.7 years) High rPE values obtained from the model may be caused by yet unidentified covariate relationships, which were not taken into account in the original modeling process but do have an effect on ceftriaxone PK in PICU patients.
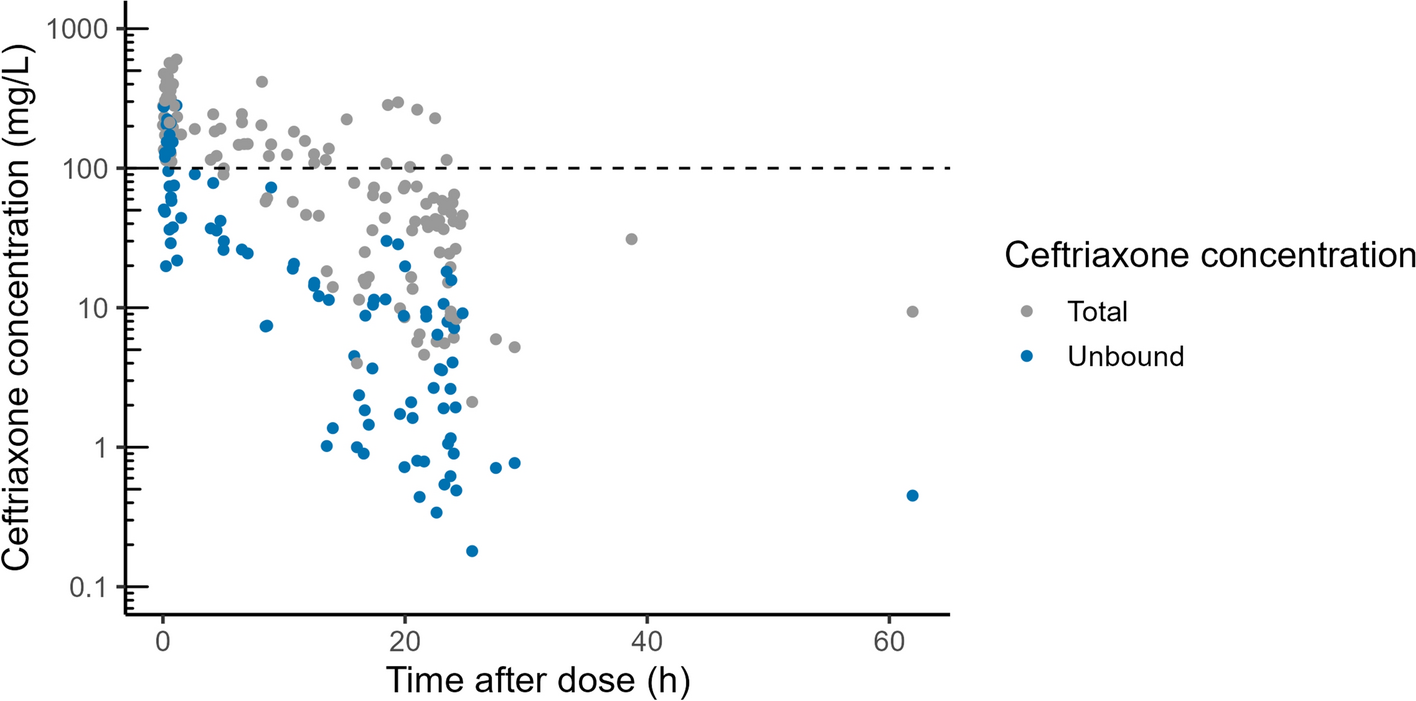
Our data presented relatively high ceftriaxone concentrations in the critically ill pediatric population. Peak concentrations up to 601.0 mg/L and a median trough concentration (20–26 h after dose administration) of 37.8 mg/L (range 2.11–262.7 mg/L). These results illustrated high ceftriaxone exposure among our study population, well above the current clinical breakpoint minimal inhibitory concentration (MIC) of 0.125 mg/L or above the cutoff value for dose reduction (10 times > MIC) [26]. Ceftriaxone is often used in the treatment of meningitis, and a higher ceftriaxone serum concentration is associated with higher penetration through the inflamed blood–brain barrier (BBB) [27]. However, ceftriaxone treatment is associated with possible life-threatening conditions, as illustrated by Lacroix et al., who described serious central nervous system (CNS) adverse drugs reactions (ADRs) leading to mortality [15]. Two cases of CNS ADRs in pediatric patients were reported (age 8 and 12 years). Of all the studied case reports, 9 out of 19 reported trough concentrations above 100 mg/L (none of the children) with a median value of approximately 75 mg/L. Trough concentrations of total ceftriaxone above 100 mg/L are associated with CNS ADRs in high-dose regimens [28]. A recent case report describing a 4-year-old girl with cephalosporin-related neurotoxicity showed total and unbound ceftriaxone trough concentrations of 130 and 33.9 mg/L [29]. All in all, there exist only a few reports of ceftriaxone-induced CNS ADRs in children. This poses the question of whether CNS ADRs often go unrecognized in critically ill pediatric patients owing to concurrent multiorgan dysfunction, intubation, or sedation. Ceftriaxone toxicity is frequently reported in the elderly population, indicating that cerebral frailty or impaired renal function may increase susceptibility [28]. More awareness needs to be created toward ceftriaxone CNS toxicity in fragile populations. All in all, dosing of ceftriaxone poses a critical balance—high serum concentrations for BBB penetration and trough concentrations < 100 mg/L—to prevent AEs. These findings may suggest that additional research is required that distinguishes dosage regimens (i.e., bloodstream infections from meningitis), as patients with bloodstream infections may not require a high dosage to achieve sufficient BBB penetration. In case of meningitis or infections requiring high antibiotic target site concentrations, the available dosing regimens should be applied. In addition, PopPK models may be used to predict the individual concentration-time profile and perform MIPD to provide dosage adjustments, taking the patient’s indication into account. These methods may be supported in the future by prospects such as ADR prediction models constructed by machine learning using electronic patient records [30].
This study has some limitations. Although data inspection was performed prior to model evaluation, errors might remain in the dataset owing to time registration. The effects of incorrect registration of sampling times on model performance has been described earlier [31]. Furthermore, patient values for PHDI and HITEMPDI (model-specific indicators used to account for the effects of pH and temperature, respectively, as referenced in Tang Girdwood et al. [5]), and PRISM3 were not available. This may have impacted the estimation of the corresponding individual PK parameters. However, it was demonstrated in our analysis that adequate population predictions could still be obtained irrespective of the missing covariate values. All in all, it is likely that the predictive performance was reduced by the missing covariates. Covariate relationships from the Tang Girdwoord et al. model were fixed to 0 (except creatinine clearance (CRCL)). Tang Girdwood et al. included the PRISM3 score as a covariate on clearance of the unbound ceftriaxone fraction. The obtained parameter estimate for PRISM3 (–0.0142) indicates a small stepwise decrease in renal function for increasing PRISM3 scores. Both covariates, PHDI and HITEMPDI, exhibit small effects on ceftriaxone clearance (±15%) for the total and unbound ceftriaxone concentrations. In addition, recapture of the models was based on published code or received model codes, as the original NONMEM model code was not available for all included models. However, complicated interpretation of published NONMEM models led to the exclusion of one ceftriaxone popPK model. The original model codes were available for the models from Hartman et al. and Tang Girdwood et al. [3, 5]. As the authors did not specify coping with below the LLOQ concentrations, caution is required when interpreting concentrations below the publication specified LLOQ. Patients who were included in the EXPAT Kids study were sparsely sampled, since most often one sample per dosing interval was available. There are no formal standards for assessing the performance of popPK models in external validation. However, several recent publications set threshold values to evaluate a previously developed popPK model (MDPE ≤ 15%, MAPE ≤ 30%, F20 > 35%, and F30 > 50%) [19, 20, 32]. Some models fulfilled these new standards (F30 and F20 criteria), providing confidence in using these as criteria for acceptability [32]. In this paper, we focused on the criteria for both PRED and IPRED values. However, relying solely on IPRED values can be misleading owing to improved fit and potentially masking inadequate population PK parameter values. Adequacy of the latter is essential to describe the characteristics of the population from the external dataset. Therefore, meeting the performance criteria for PRED values is of higher importance than for IPRED values. Not all evaluated models were developed using data from critically ill PICU patients, which may have decreased model performance. For instance, the models by Wang et al. and Khan et al. tested serum creatinine as a covariate relationship, without results (Hartman et al. and Tang Girdwood et al. did manage to include eGFR). This may be explained by the lack of included critically ill patients with kidney dysfunction in the studies of Wang et al. and Khan et al. Lastly, the external dataset was based on a small group of subjects. This might not be representative of all pediatric patients, as pediatrics encompasses a large population with variable PK parameters. However, significantly larger sample sizes might not be required to perform an external validation [33].
Ceftriaxone is a frequently used antibiotic for the treatment of meningitis and other severe infections. However, studies describing the PK of ceftriaxone in the critically ill pediatric population are scarce. In this study, several published popPK models have been externally validated to compare PK predictions in the complex PICU population. Only the model by Khan et al. managed to satisfy all criteria for model performance; predictive performance varied widely among models and tended to overpredict. Our external dataset comprised high ceftriaxone trough concentrations, indicating that the current dosing regimens for ceftriaxone may need to be re-evaluated to minimize the risk of overdosing and prevent serious CNS ADRs in this fragile population. Future research should focus on the fine dosing balance for ceftriaxone (especially in patients with meningitis), considering adequate exposure but preventing high trough concentrations. Clinicians and pharmacists should be cautious when applying popPK models for MIPD, as adequate model performance is not guaranteed. In the future, advanced methods (such as model averaging/ensembling/re-estimation) could be considered to more accurately predict an optimal individual dosage for critically ill children.


Comments (0)