4.1 Main Findings
Our kinetic model used fluid-induced plasma dilution as the input variable and re-created this variable with good precision (Fig. 2). Plasma dilution is the most widely used surrogate measure of plasma volume expansion. When reviewing the volume kinetics of Gelofusine as a whole, very little resembles the kinetics of crystalloids. The behavior of the fluid in the body is more like that of fluids that contain larger colloid molecules.
Gelofusine occupied the intravascular space, and only a smaller fraction (15%) resided extravascularly. Elimination occurred with a half-life of almost 2 h, which was substantially shortened with noradrenaline. This half-life was virtually identical to the 116 min previously reported for Voluven in volunteers [11] but still much shorter than the 22 h reported for albumin 20% during surgery [12]. The elimination of crystalloids admittedly occurs more slowly in the anesthetized than in the awake state [5], but the rate of distribution of crystalloid fluid is approximately 50 times higher than the rate reported here for Gelofusine, which still makes the dilution–time curves profoundly different.
Simulations based on the kinetic parameters show how Gelofusine can be administered to achieve a steady state plasma dilution during vascular surgery associated with minor hemorrhage. An initial rapid infusion over 20 min creates a plasma volume expansion 20 times the infusion rate in mL/min, which can be maintained over time by reducing the infusion rate to as little as 15–20% of the initial rate (Fig. 4).
4.2 Noradrenaline
Administration of noradrenaline had a profound influence on the kinetics of Gelofusine and consisted of increased elimination of plasma water (higher k10) and a temporary expansion of the interstitial fluid space (higher k12 and k21). Hence, noradrenaline influenced the extravascular space in two phases, first hydration and second volume depletion.
A decreasing effect of noradrenaline on the plasma volume (lower Vc) and the accelerated elimination rate reported here have previously been found when noradrenaline was administered and albumin 20% served as infusion fluid during surgery [12]. Hemoconcentration as evidence of vascular contraction has also been reported when noradrenaline is administered to volunteers [14] and to patients requiring noradrenaline to reach an acceptable MAP [15].
The kinetic parameter k21 is believed to mainly represent the lymphatic flow, which is influenced by the adrenergic balance [16]. The strong positive covariance between exogenous noradrenaline and k21 in the present study is supported by experiments in sheep demonstrating a five-fold increase of the lymphatic flow in response to administration of this catecholamine [17]. As shown in Fig. 3C, the influence of noradrenaline on k21 helped to remove distributed fluid from the extravascular space during the later stages of the study.
The fact that noradrenaline was administered to 8 of the 15 patients does not confound the conclusions. The kinetics without noradrenaline are given by the typical values (tv) of the parameters in the base model, shown in Table 3, and the kinetics with noradrenaline are given when considering the modifications of the parameters prompted by the covariance values. Calculation of the covariances was based on all 280 data points because noradrenaline operated as a “time-varying covariate”, which means that a new value for the relationship was obtained for each point in time when the dose of noradrenaline was recorded, and plasma dilution was measured.
4.3 The Oncotic Pressure and Physiology
Translating the current findings to physiology is partly possible but should not be taken too far. The kinetic parameters are functional entities but are often softly explained in physiological terms because infusion fluids do not metabolize or bind to tissue [5]. In the present study, the oncotic effect of the administered gelatin molecules needs to be discussed.
The oncotic pressure of Gelofusine is 39 mmHg [18], whereas that of plasma is 25 mmHg [17]. Slight hyper-oncoticity is needed to counteract the fluid-induced increase in capillary hydrostatic pressure, which accelerates capillary filtration. The oncotic pressure of Voluven is 33 mmHg, which seems to balance out the hydrostatic pressure effect. Infusion of Voluven in volunteers yielded a Vc of 3.1 L, which agreed perfectly well with anthropometric predictions and supports that extravascular fluid was not recruited [11]. Therefore, a slight hyper-oncotic effect of Gelofusine remains, but it is far from albumin 20%, which has a colloid osmotic pressure of 160 mmHg [13].
4.3.1 Central Fluid Volume
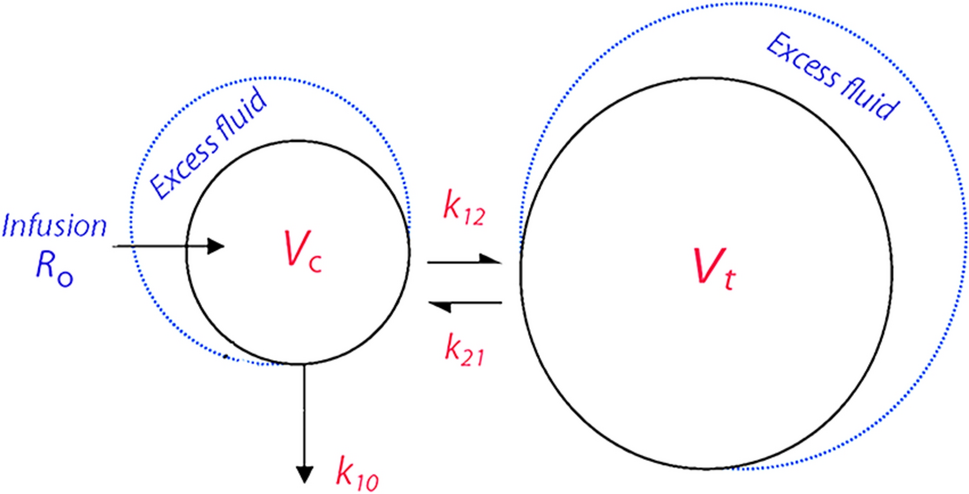
The parameter Vc quantifies the relationship between the measured plasma dilution and the corresponding volume expansion. Thus, it corresponds to the central volume of distribution in drug pharmacokinetics. Vc usually attains a size close to the expected size of the plasma volume except in association with sharp shifts of the Starling forces [19]. In the present study, Vc averaged 2.16 L. A value closer to the anthropometric value of 2.95 L would be expected, but Vc was in fact 0.76 ± 0.53 L smaller.
This discrepancy can be explained by low fluid intake and chronic medical therapy. Other explanations include recruitment of extravascular fluid to the plasma due to anesthesia-induced hypotension [20] or hyper-oncoticity of the infused fluid [21]. Transfer of extravascular fluid to the plasma decreases the reported Vc in volume kinetic analyses, which might be counterintuitive because Vc is also low in hypovolemic states [22].
Post hoc simulations suggest that fluid recruitment due to anesthesia-induced hypotension or hyper-oncoticity could have amounted to a maximum volume of 300 mL if they were the sole cause of the low Vc. In studies of albumin 20%, we have normalized Vc after considering the oncotic-driven fluid recruitment from the extravascular space to the plasma by adding an absorption function to the model where the rate of uptake is modified by the increase in plasma albumin or the plasma oncotic pressure from baseline [12, 13]. However, in the present study, an absorption function did not attain statistical significance, which suggests that the recruited fluid volume, if any, was small.
4.3.2 Rate Constants
The rate constants reported in volume kinetics cannot be directly translated to specific physiological mechanisms that govern fluid distribution but rather as summary measures of variables commonly reported in physiology. The Starling equation holds that the increased transcapillary filtration resulting from volume loading is the combined effect of plasma protein dilution and increased capillary hydrostatic pressure. In volume kinetics, these time-varying forces are summarized in the volume expansion of Vc, as volume expansion both dilutes the plasma proteins and increases the hydrostatic pressure.
The static resistance to filtration in physiology is the reflection coefficient, which, together with the surface area available for filtration, is represented by k12 in volume kinetics. We speculate that the plasma oncotic pressure becomes a static force when a hyper-oncotic fluid is infused because every incremental decrease of this pressure is followed by increased capillary filtration. In studies of albumin 5%, the increased plasma albumin level attained steady state for several hours, whereas the plasma volume decreased [13, 23]. Similar findings have been made with albumin 20%, where steady state for the plasma colloid pressure has even been demonstrated [13]. Thus, hyper-oncoticity is considered by the rate constants, which are low but not flawed, whereas the fluid-induced increase in capillary hydrostatic pressure remains the only time-varying driving force for filtration.
4.3.3 Urine Flow
Urinary excretion is routinely used to stabilize the calculations in volume kinetic analyses of crystalloid fluid. This approach worked poorly for Gelofusine, as has been the case for other colloids of similar oncotic strength [11, 23]. The gradual decrease in plasma-volume-expanding effect of a colloid fluid is due to complex events that involve rapid renal excretion of the smallest molecules, and larger ones are subject to capillary leakage as well as gradual enzymatic degradation.
In our study, the modelled elimination clearly exceeded the measured urine output. The fate of the excess of eliminated fluid is unclear; some of the volume could have evaporated or leaked into the operating field but without being in balance with the plasma. This discrepancy cannot be explained by oncotic withdrawal of fluid as that would have the opposite effect.
4.4 Pharmacology
Gelofusine contains a spectrum of gelatin molecules with an average weight of 30 kD, which is small enough to be excreted by the kidneys. However, the succinylation increases their molecular size, which makes the weight somewhat misleading. The smallest molecules are still excreted by the kidneys, and the larger ones are gradually degraded in the liver until they are also excreted by the kidneys. Only a small fraction is completely metabolized. The production information accompanying Gelofusine states that the molecular kinetics has two phases: the first has a half-life of 8 h and the second a half-life of several days. Hence, the half-life of the gelatin molecule should not be confused with the half-life of the infused volume. However, the half-life of the fluid in the body, as given by the measured urine output, would be somewhat longer.
4.5 Clinical Studies of Volume Expansion
Clinical literature about gelatin as an infusion fluid is sparse. Lobo et al. [4] infused 1 liter of Gelofusine and Voluven over 1 h during laparoscopic cholecystectomy and measured the hematocrit at hourly intervals. They estimated that the BV was increased by 70% of the infused amount, but the expansion was more sustained with Voluven. The calculations did not account for elimination.
The same group also studied Gelofusine and Voluven in volunteers and concluded that Gelofusine does not cause metabolic acidosis; the chloride concentration is 120 mmol/L in Gelofusine and 154 mmol/L in Voluven. Both fluids increased the brain natriuretic peptide concentration and decreased plasma renin, and the maximum plasma volume expansion after Gelofusine was 60% of the infused volume [24].
Dubniks et al. [25] infused colloid fluids in rats and found that 5% albumin provided greater plasma volume expansion than Gelofusine and Voluven when measured with a radioactive tracer 2 h after a 1-h administration of these fluids. This difference agrees with findings in humans where 5% albumin has an intravascular persistence half-life of 6.5 h [13].
Volume expansion might be monitored clinically by measuring hemoglobin noninvasively. The bias was numerically large when examined during fluid loading with Gelofusine [26], hydroxyethyl starch [27], and Ringer’s solution [27], but it was much lower when considering changes in hemoglobin rather than absolute values [26, 28].
4.6 Safety of Gelatin
Gelatin has had a bad reputation for some years because of the risk of spreading “slow virus” (prion) diseases such as “mad cow disease”. To prevent this problem, gelatin preparations are now heated to high temperatures before sale.
Current safety concerns include anaphylaxis, bleeding, and renal failure, for which the literature provides mixed conclusions. Anaphylaxis is more common than with other colloids [1, 29]. The reactions are usually mild and consist of erythema or urticaria, but severe reactions do occur [29]. The effect on coagulation is mild [2], although slightly aggravated surgical hemorrhage has been reported [30]. Most studies have not disclosed increased risks of kidney injury of death post-infusion [31,32,33], although these issues may not be finally settled.
The past decade has added only a little to the literature but includes that Gelofusine might protect the kidneys from nephrotoxic drugs such as polymyxin B [34].
4.7 Benefits and Limitations
The current study reports the first kinetic analysis of the volume effect of gelatin over time. The observations were quite consistent even though the study was performed during ongoing surgery in patients with ASA scores of III. We believe they can be generalized and should be considered when Gelofusine is used in the clinic. The results also provide a basis for administrating Gelofusine in ways that expand the plasma volume without marked variations over time.
The limitations of the study include the fairly low number of patients. They were sufficient for confidently estimating the kinetic parameters in the base model but did not offer enough statistical stability for quantifying some covariate effects that were on the verge of being significant. One variable that was close was the urinary creatinine concentration, which is a measure of renal water conservation but mostly reflects preoperative hydration status [7]. High urine creatinine before surgery slows the elimination of albumin 20% [35] and crystalloid fluid [36]. Another variable was MAP, which strongly affects the elimination of crystalloid fluid [37].
Two patients were classified as emergency cases based on the surgical team’s decision. One involved an unruptured popliteal aneurysm that had recently increased in size, and the other was a case of cerebrovascular disease with recent contralateral temporary numbness. These cases were included because the surgical times were expected to be short and without the need for blood product administration, which could confound the interpretation of Gelofusine volume kinetics.
The size of the peripheral fluid space (Vt) was much larger than the ECV estimated by anthropometry. The reported size is even unphysiological, which might suggest an absence of the free flow of excess fluid in Vt. The flow of fluid is known to be restricted in the gel phase, which makes up most of the interstitial space [38]. However, the estimate could also have been confounded by the strong dependency of Vt filling on noradrenaline, which was only administered to half the patients and at variable rates.
The kinetic analysis did not account for blood loss (mean 50 mL) or evaporation. These variables affect the hemodilution in opposite ways and are likely to cancel each other out: blood loss decreases the hemoglobin level, whereas evaporation increases it. Early work with volume kinetics considered both factors, but their inclusion only influenced the kinetic parameters when there was major hemorrhage [39]. Moreover, the capillary leakage and lymphatic return flows at baseline (about 6–7 mL/min) are not included as they normally cancel out.
Maintenance fluid was withheld during the study, but the patients were constantly and modestly hypervolemic because the infused Gelofusine was believed to markedly exceed the hemorrhage volume and possible preoperative hypovolemia. Hence, the low MAP that motivated noradrenaline administration was more likely to be due to an anesthesia-induced increase of the venous capacitance than to absolute hypovolemia [40].


Comments (0)