Population Pharmacokinetics of Tarlatamab, a Half-Life Extended DLL3-Directed Bispecific T-Cell Engager in Patients with Previously Treated Small Cell Lung Cancer
Background and Objective
Tarlatamab is a first in class, half-life extended delta-like ligand 3 (DLL3) directed bispecific T-cell engager (BiTE®) immunotherapy that has shown durable efficacy in patients with previously treated small cell lung cancer (SCLC). The purpose of this analysis was to develop a population pharmacokinetic (PK) model for tarlatamab.
Methods
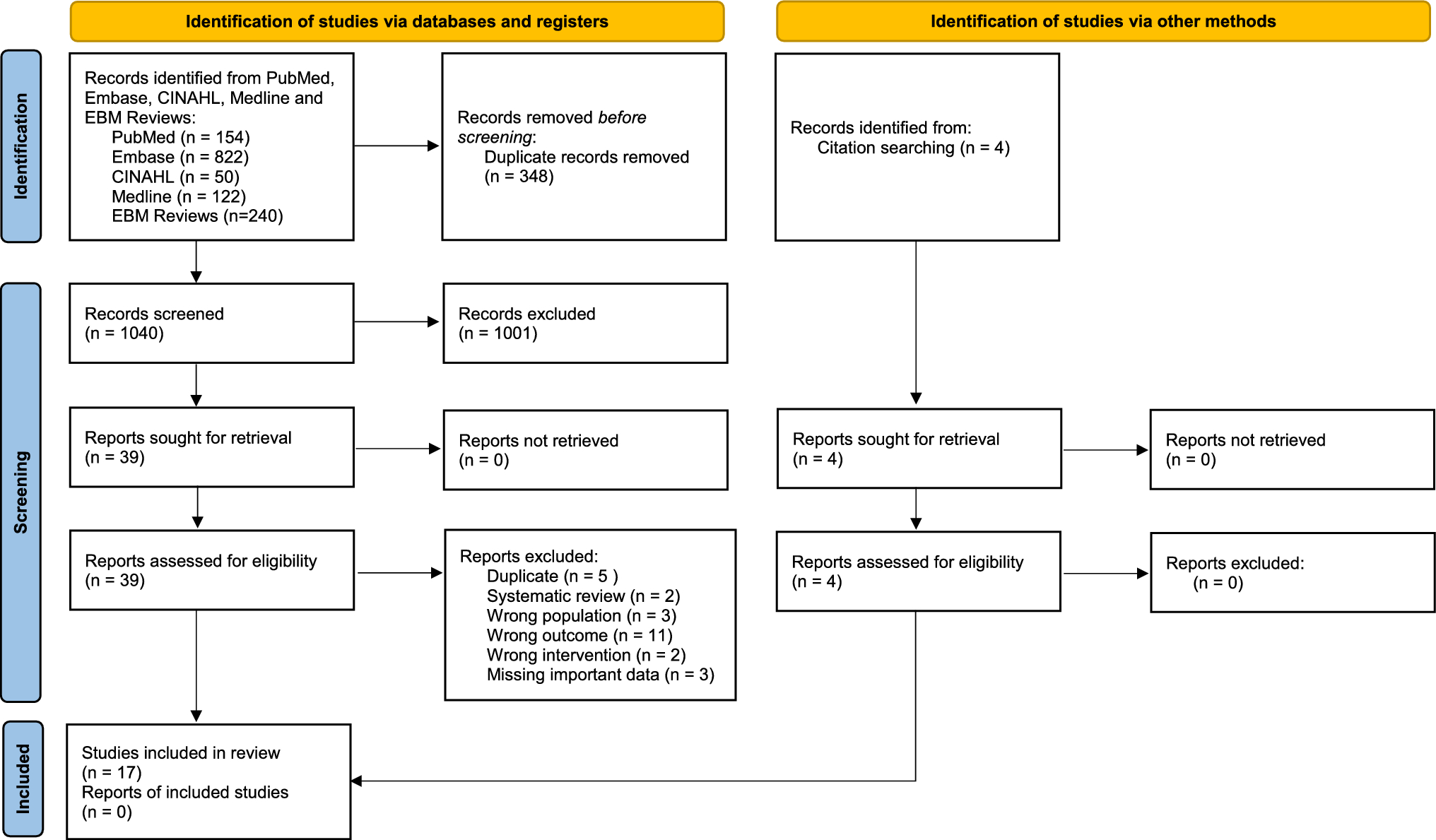
This analysis includes data from 420 patients with previously treated small cell lung cancer (8509 samples) pooled across the Phase 1 DeLLphi-300 study (dose range 0.003–100 mg every 2 weeks and 200 mg every 3 weeks) and Phase 2 DeLLphi-301 study (10 mg and 100 mg every 2 weeks). The data were analyzed using a nonlinear-mixed effects modeling approach implemented in NONMEM (v7.5) software and validated using standard statistical approaches. The effects of intrinsic and extrinsic factors on PK parameters and exposures of tarlatamab were evaluated, and the impact of identified covariates were further assessed using simulations.
Results
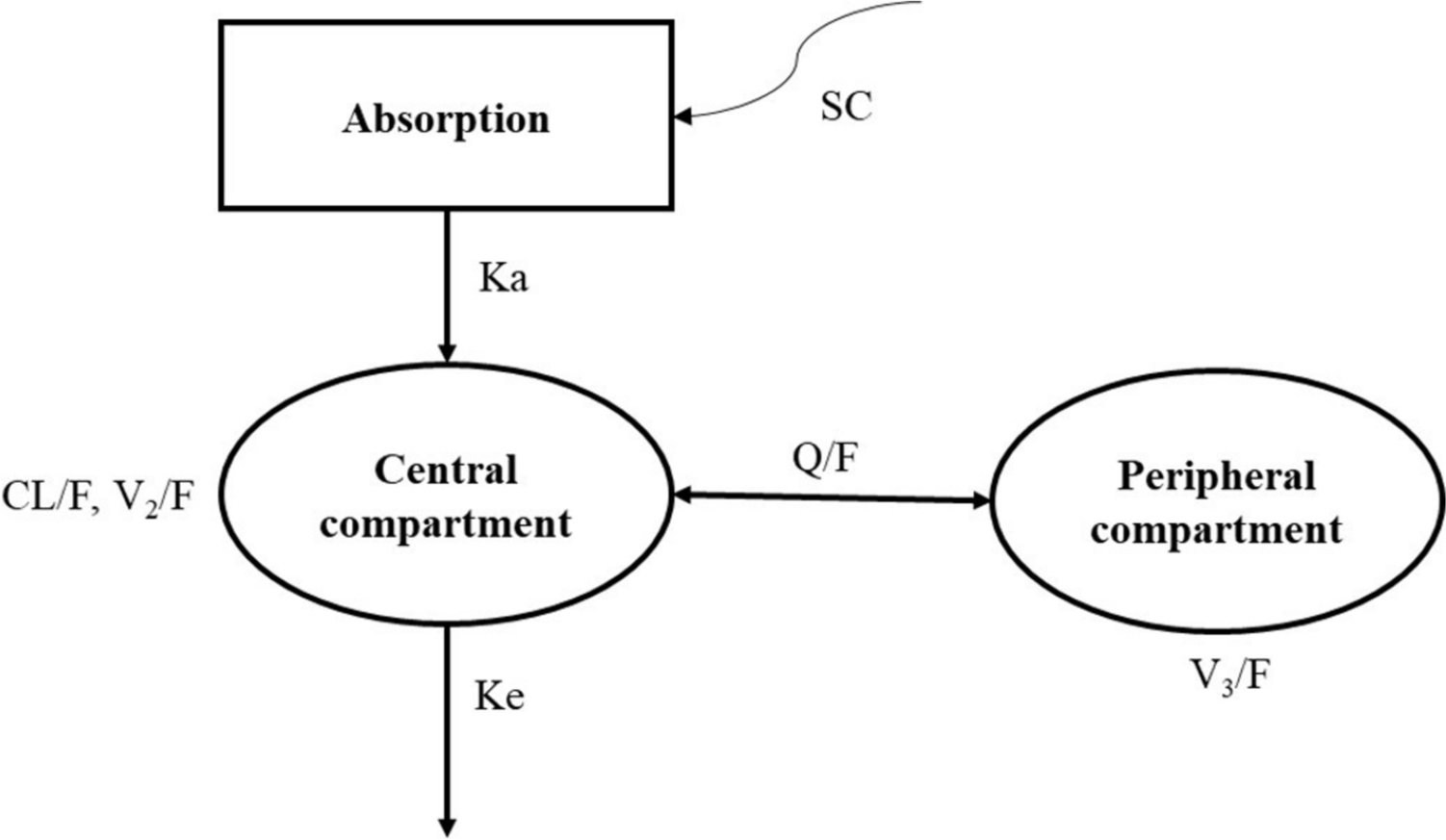
Tarlatamab serum concentration data were best described by a two-compartment model with linear elimination. Tarlatamab clearance (CL) and central volume of distribution (VC) were 0.649 L/day and 3.44 L, respectively, for a typical 73-kg individual. The model-estimated median terminal phase elimination half-life was 11.2 days. Tarlatamab pharmacokinetics were not impacted by age, sex, ethnicity, estimates of renal and hepatic function, prior lines of therapy, or baseline disease status. The presence of antidrug antibody (ADA) at any time during the study and bodyweight were found to be statistically significant covariates on CL, and Asian race and bodyweight were found to be statistically significant covariates on VC; however, they did not lead to a clinically meaningful impact on exposures.
Conclusions
The pharmacokinetics of tarlatamab was well-described by a two-compartment model with linear elimination. No clinically significant differences were observed on the basis of age, sex, bodyweight, race, ethnicity, estimates of renal and hepatic function, prior lines of therapy, baseline disease status, or emergence of ADA. These results support that no dose adjustment is required on the basis of any of the evaluated covariates.


Comments (0)